Hepatitis C: "Affectionate Killer"
When we talk about severe infectious diseases that lead to death and are subject to the greatest stigmatization, we usually mean HIV. Hepatitis C is particularly notable among other diseases. Most people infected with the hepatitis C virus acquire chronic infection, which is asymptomatic and leads to cirrhosis and liver cancer, and subsequently, respectively, death. Because of these features, hepatitis C has been given the nickname “affectionate killer”.
Hepatitis C and HIV are often mentioned together, and this is not an accident: today they are the most dangerous rapidly spreading infectious diseases. Both of these diseases are transmitted through blood contact; however, hepatitis C infection through sexual contact is much less likely.
A bit of history
The infectious nature of certain liver diseases was discovered by S. P. Botkin in the 19th century: the disease he described today is called Hepatitis A; the next described, respectively, hepatitis B. After the isolation of the pathogens of these diseases, it became clear that they are not the only ones, there is hepatitis “neither A nor B”. The RNA of the causative agent of this disease, hepatitis C flavivirus, was detected in 1989 in the blood of patients.
In a large number of cases, hepatitis C is asymptomatic, and a person may be unaware of his illness for many years. Laboratory method - the only way to reliably determine the presence of infection. To determine the presence of infection, an antibody test (Anti-HCV-total) is used, if the result is positive - PCR and genotyping.
Over time, the disease leads to liver fibrosis (the degree of fibrosis can be determined using elastometry). The degree of F0 is the absence of fibrosis, F4 is cirrhosis. Further progression of the disease leads to the inability of the liver to perform its functions (decompensated cirrhosis) and the development of liver cancer.
Interferon therapy
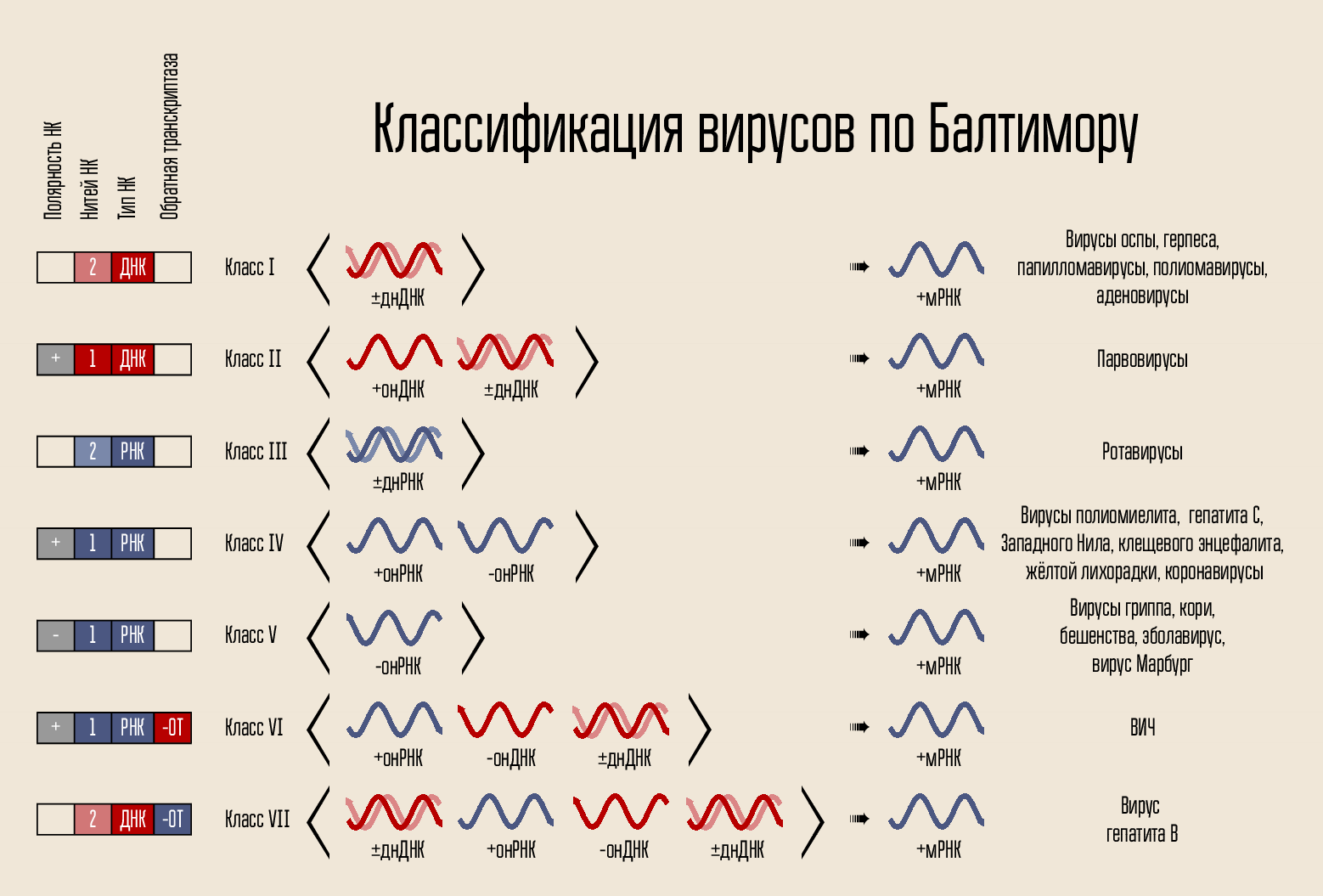
Hepatitis C virus is an RNA-containing virus, in the life cycle of which there is no DNA phase. Accordingly, its genetic material cannot be stored indefinitely inside the cell nucleus (as HIV does, for example). This greatly simplifies the approach to treating the disease - if replication of the virus is suppressed for some time, then a complete cure is possible.
Interferon therapy (interferon alpha-2a) and ribavirin was the first successful approach to treating the disease.
Interferons are proteins that the body produces and that by themselves do not know how to fight infection. They activate the defense mechanisms in the cells, and that is why the side effects of the use of interferon resemble a flu-like state - the body „considers“ that it is sick and begins to fight the infection with the methods available to it. To increase the period of interferon in the body, it is associated with polyethylene glycol (pegylation).
Another component of this therapy, ribavirin, is similar to the nucleosides adenosine and guanosine. It consists of sugar (D-ribose) and parts, similar to the purine nitrogenous base, but not being them. Viral polymerase tries to build RNA complementary to the RNA of the virus, but cannot, because it uses ribavirin instead of the desired nucleosides.
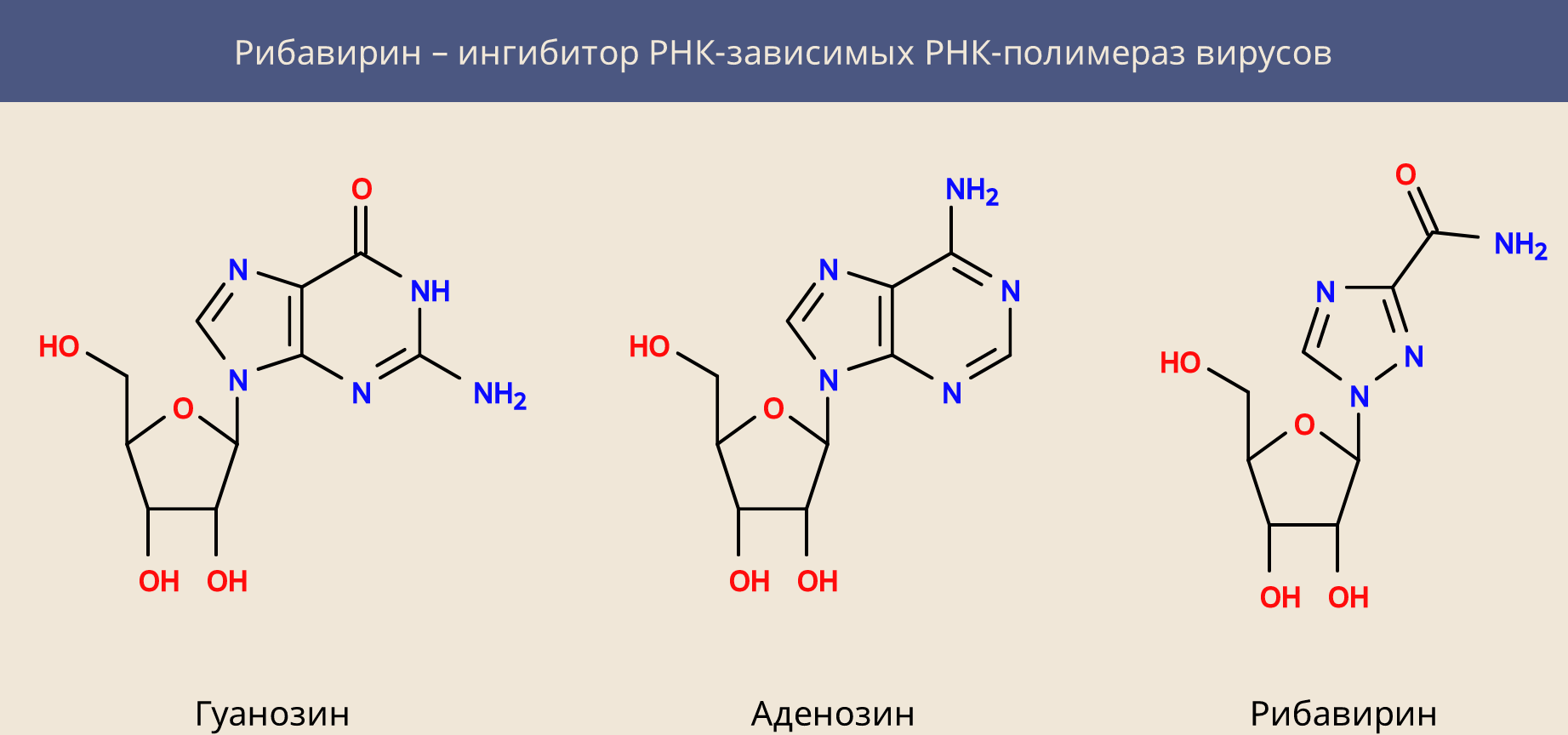
Ribavirin is not a specific cure for hepatitis C, it is active against many other RNA-containing viruses, disrupting the process of rewriting their genome. However, it has another property: it inhibits inosine monophosphate cell dehydrogenase and reduces the intracellular concentration of guanosine triphosphate. This explains both its activity against DNA-containing viruses, and its general cytotoxicity.
Interferon therapy
Unfortunately, interferon therapy could (depending on the genotype of the virus) cure only 45 to 70 percent of patients. Today she was replaced by direct, interferon-free therapy.
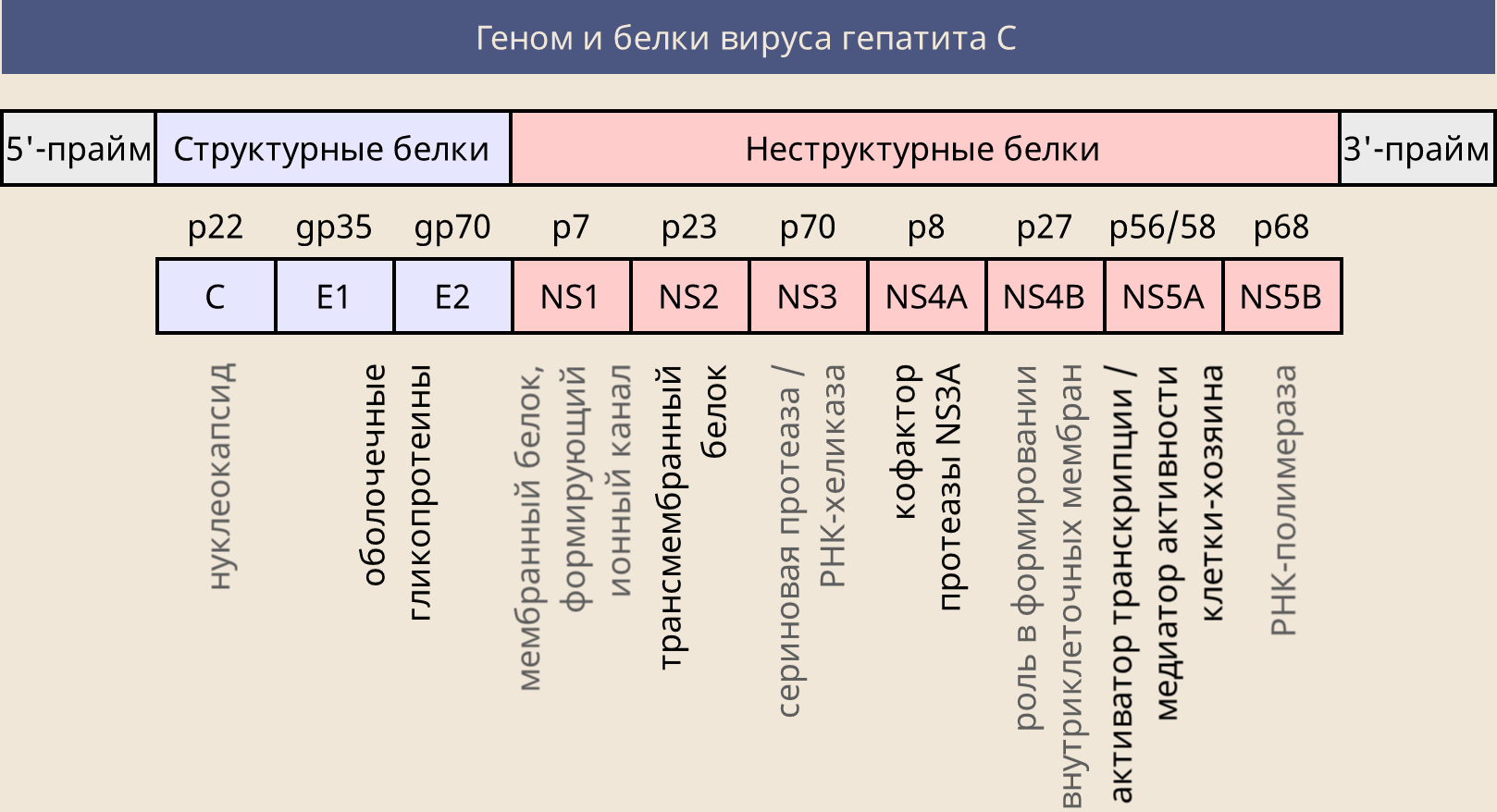
Hepatitis C virus RNA encodes several proteins necessary for the virus to complete its life cycle. These include the structural proteins E1 and E2 (necessary for assembling the shell of the virus) and non-structural NS (performing certain functions).
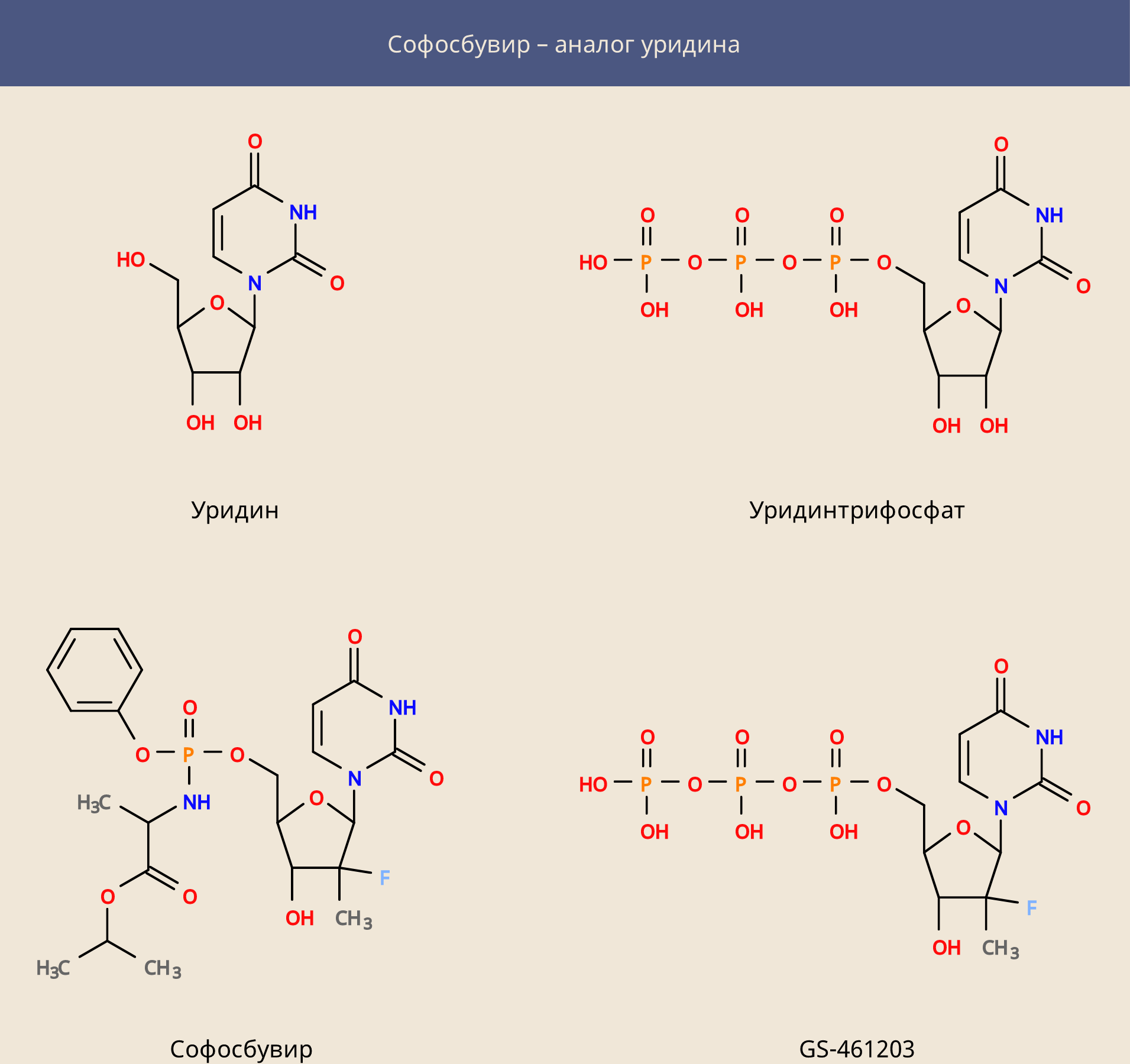
The first target of the attack (as for ribavirin) was the NS5B viral polymerase, but this time it was able to attack it more directly by creating an analogue of the uridine nucleoside, sofosbuvir. This prodrug is similar in structure to uridine monophosphate, to which additional parts are attached - these parts allow it to freely enter the cell, where with the help of cellular enzymes, sofosbuvir is converted to a metabolite GS-461203 (triphosphate).
Sofosbuvir turned out to be in itself an extremely effective medicine, but could not cure all cases of infection. Today, there is a large set of drugs, which in most cases can cure hepatitis C.
In addition to NS5B polymerase, the goals of anti-hepatitis C drugs are:
- NS5A protein, which has no direct enzyme activity, but plays an important role in the life cycle of the virus (the names of the drugs end in -asvir, typical examples are Ledipasvir and Daclatasvir). Sofosbuvir + Ledipasvir and Sofosbuvir + Daclatasvir are highly effective;
- NS3 viral protease and its NS4A cofactor (drug names end in –previr, for example, simeprevir). According to the latest treatment guidelines for hepatitis C, the use of protease inhibitors is not recommended for decompensated cirrhosis.
What medicines will not help, and how to choose the right ones?
Only the above types of drugs will help. No hepatoprotectors and folk remedies will help to get rid of hepatitis C. The use of interferon-free regimens shows a much higher cure rate and fewer side effects, but, for example, in Russia, the reality is that the patient in most cases has to take care of buying the drugs.
The correct treatment regimen and its duration should be selected exclusively by an infectious disease doctor . He is guided primarily by the degree of liver fibrosis and what is the genotype of the virus (since the definition of the genotype of the virus may malfunction on recombinant types, the use of pangenotypic drugs is recommended), but not only. An important role is played by the compatibility of drugs with others that the patient takes, the presence of co-infection with HIV and / or hepatitis B, kidney function, and much more.
Unfortunately, the vaccine against hepatitis C does not yet exist, but the disease is curable - the main thing is to start therapy on time, before the onset of serious consequences.
')
Source: https://habr.com/ru/post/451332/
All Articles