Direct comparison of laser myopia correction methods or what you pay for when choosing ReLEx SMILE
We “fixed” Boomburum with a laser here , and in a post where he talked about his new eyes, there was a discussion on the comparison of the PRK-methods, LASIK-methods and SMILE-methods. We (I mean the German holding SMILE EYES , which includes our Russian clinic) do all three types of operations, but absolute supporters of the method that will give more if you lose less. Thus, any kind of LASIK or PRK is recommended only when SMILE is impossible: firstly, with hyperopia (this is a completely different story), secondly - in cases of a diseased or damaged cornea (for example, with scars). But, of course, the economic side is taken into account.
It would seem that in the first posts I explained why. But in the comments to the post it is clear that this was not enough. Therefore, let's do everything according to the rules of scientific discussion. Let us analyze theses and bring the relevant research to them.
That is what they do in the scientific and medical world. If you have an opinion, you need to justify it. Preferably, a sample of 20 or more patients with the same distribution in a double study. It is desirable that research be confirmed by different clinics in different countries where such types of operations are performed.
')
Let's start.
We define the terms
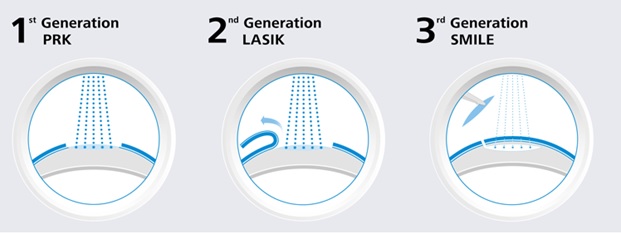
SMILE (ReLEx SMILE or hereinafter simply SMILE) born in 2007 - Small incision lenticular extraction - 100% femtosecond technology. The prefix Femto- means that the laser has a very short pulse: 10 15 pulses fit in every second. At the same time, the coherence and power of the outgoing beam is maximum. With its help, a three-dimensional cut of the “shape” in the form of an individual lens — the lenticules inside the cornea and its removal through a small entrance (1.5–4 mm) occurs. The “figure” from the inner layer of the cornea is microinvasively extracted — nothing is evaporated, and the cornea acquires a new form. Here are the details. Here is the principle of operation , and here the operation itself. Inside SMILE EYES holding - 0.5% for enchancment (additional correction), in the world - up to 2%.

This is how ReLEx SMILE is performed.
FLEX , born in 2005, is the predecessor of the SMILE method, also 100% femtosecond technology. Now it is fashionable to sell it as a "pseudo-Smail". The difference is that, like SMILE, an individual lens is cut into the cornea, but a flap is cut to remove it around the circumference. That is, there is no heating and evaporation - this is a plus, but otherwise - the same opening of the “cover”. It is done under a single laser, excimer is not needed. Does not give the patient significant advantages over femtoLASIK. The equipment manufacturer offers it as part of preparing the surgeon for the SMILE method.
femtoLASIK (FS-LASIK, femtosecond LASIK) 2000 year of birth - a method using necessarily two lasers: a femtolaser and an excimer laser.
A femtolaser is used to form a “lid” in the cornea, then the lid is folded manually. For evaporation of the lens in the middle layers of the cornea, an excimer laser is needed. There is a thermal effect. The operation depends on the quality of each of the two lasers (old models of both the one and the other can spoil the overall result). Then the lid fits into place. It never grows, you can always pick it up. The purpose of the operation is not to burn over the upper layers of the cornea, which are the most durable and contain the greatest number of nerve endings. Now it is one of the most common operations in Russia and in the world. Inside the holding is only about 5-10% of the entire correction of myopia. Statistics on the additional correction in the world - 8-12%.
The term "SUPER-LASIK" - not a separate method - is used as a characteristic of evaporation profile by an excimer laser - it means an individual evaporation profile in the cornea. That is, it can be either "SUPER-femtoLASIK" or "SUPER-just-LASIK". In scientific medical publications, the term "Super Lasik" (with the prefix "Super") is not used and is not official medical terms. It has gained some popularity in the advertising of some medical clinics, apparently wishing to draw additional attention to themselves at the expense of "bright terminology."
LASIK (Laser-Assisted in Situ Keratomileusis) - born in 1989 - surgical separation of the flap cover using a microkerate device, a special machine with a “shaving” blade and subsequent excimer laser evaporation of the lens on the cornea. For evaporation of the lens in the middle layers of the cornea, one laser is needed - an excimer and mechanical device by a microkeratome. LASIK - a combination of mechanical and laser effects. The result depends on the quality of the laser and the quality of the microkeratome. There is a thermal effect.
All its varieties are also morally obsolete: the Epi-LASIK technique - an attempt to reduce the thickness of the corneal section - indicates that the cut is made on the very surface of the cornea and the REIK technique - “horseradish is not sweeter” - this is the same LASIK. By the way, thin flap "frowns" stronger and "flies" when injured easier.
The flap also becomes the “culprit” of additional optical aberrations that affect the postoperative vision quality.
In our clinic today, a microcoratome is “shrouded” as an exhibit, for modern surgical practice this is already barbarism. It is extremely rarely needed, for example, to cut through the scars.

LASIK / femtoLASIK Scheme
PRK (Photorefractive keratectomy, PRK) - born in 1985 - a method of evaporating the lens in the upper layers of the corneal stroma without creating a flap with preliminary removal of the surface layer of the epithelium. The oldest method of all laser correction methods.
Complications are well studied, the largest statistics on them - up to 15%. Within 1-1.5 diopters of correction, it shows itself well, with a higher myopia - all disadvantages crawl out. Due to the difficult healing, the large wound surface and the risks, it can only be recommended for economic reasons.
Of the minuses - the huge cornea surface (πR2 - area!) “Evaporates”, it is important that the strongest surface layers are destroyed, the border Bowman's membrane evaporates, the tissue evaporates just as much as with LASIK, scarring is possible with the appearance of persistent opacifications - heyas.
The cornea has a layered structure: epithelium, bowman membrane, stroma, Descemet's membrane, posterior epithelium (endothelium). Stable refractive effect is achieved only when the geometry of the stroma (the main layer of the cornea) changes. Achieving the stroma is a serious problem, so all varieties of PRK differ in the way they “pass” the first two layers: the epithelium and the bowman's membrane. The old “classical” method mechanically removed the epithelium - scraped off the surface. There is the option of chemical exposure to 20% alcohol solution - and then scrape. Then it will be LASEK or EPI-LASEK .
The epithelium can be “burned out” with the same excimer laser — it will be transepithelial PRK or Trans-PRK . In foreign publications, it is referred to as ASA, ASLA, C-Ten, and TransPRK. In the early years, the trans-PRK was a two-step procedure; in modern lasers, a one-step procedure.
Therefore, it is correct to say that Trans-PRK - an improved technique, but only within the framework of this method - allows reducing a number of inevitable drawbacks of the PRK method itself and errors in the results.
And the method itself, alas, cannot be called new. Although even today there are clinics that sell Trans-PRK as “the most modern method”, and sometimes “the most benign”. And PRK is in Africa PRK, even if it is “Trans.” Marketing geniuses often manage this perfectly! For example, the Estonian procedure eLASIC despite the name similar to another method is PRK.
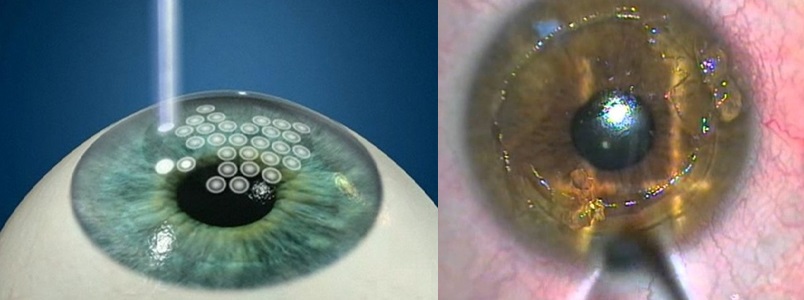
It looks like PRK
The only plus is that there is no “lid” and related problems. Well, another one - the surgeon does not need to bother to press the pedal twice and control the transitions from one software to another.
The appearance of the ReLEx SMILE method almost completely eliminated the need to perform PRK in any variants.
We have the PRK technique applied exclusively for medical reasons in cases where it is impossible to carry out the correction by other means or it is necessary to remove the upper layers of the stroma (for example, if there is turbidity).
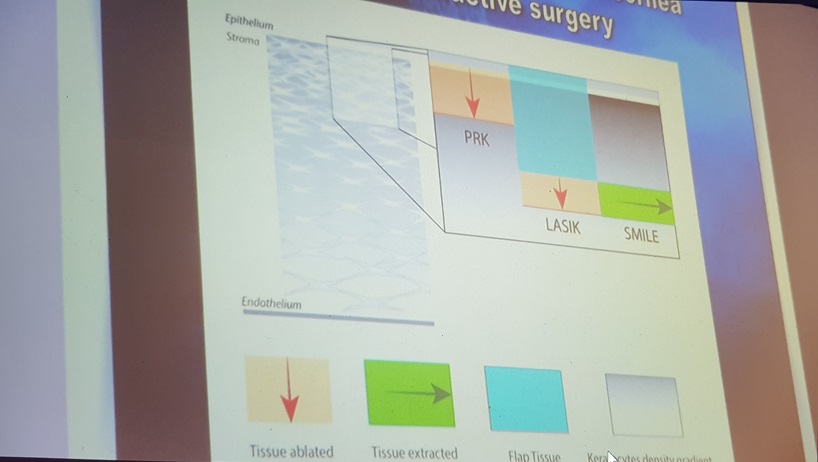
Here is a comparison of the entire range of methods.
SMILE vs PRK according to visual acuity scale
Research Nethradhama Superspeciality Eye Hospital, doi: 10.1155 / 2017/5646390.
A sample of 120 eyes from 60 patients (34 women, 26 men) who underwent bilateral correction of mild myopia (up to 4 diopters), either using ReLEx SMILE or using PRK. Visual acuity, contrast sensitivity and higher-order aberrations were recorded before surgery and compared after surgery. 3 months after surgery, a comparison was made.
Results: after 3 months, the SMILE group showed significantly better visual acuity compared to the PRK group. The postoperative spherical equivalent was comparable in both groups (SMILE = -0.15 ± 0.19 D, PRK = -0.14 ± 0.23 D, p = 0.72). However, the predictability of SE (sphero-equivalent) was better in the SMILE group — 97% of eyes within ± 0.05 D compared with 93% of eyes in the PRK group.
Higher order general aberrations were significantly higher in the PRK group compared to the SMILE group. The SMILE group showed slightly better contrast sensitivity. Four eyes from the PRK group lost one line of visual acuity due to blurring in their eyes.
Both SMILE and PRK are effective for correcting low-grade myopia. However, the SMILE procedure offered more perfect visual quality and better patient satisfaction due to greater postoperative comfort and lower aberration induction after 3 months.
My comment: when extending the sample to 6 diopters, the PRK method would lose out numerically stronger, because it gives a much higher probability of cloudiness (haze, haze) and subsequent blurring with an increase in the depth of cut. The structure of the cornea is almost always restored after a severe burn of the PRK, often they lie outside the visual area, at the borders of evaporation of the lens and have little effect on visual acuity. However, this risk is decisive in the medical choice of a method for a healthy patient without special indications. Plus, in this study, patients noted a subjective quality of life higher in SMILE-methods, since the postoperative period was painless (except for the first day).
By the way, the German refractive community Kommission Refraktive Chirurgie (KRC), as well as the German Association of Ophthalmologists (DOG), prohibits the use of PRK methods for correcting myopia with a spheroequivalent greater than -6 diopters. That is, if you have 4.5 and astigmatism is more than 1.5, you cannot do PRK! In general, choosing SMILE and the cornea will save and minimize recovery time.
But let's look at another study. It is more modern, so it was not the FRK-methods that were compared with SMILE, but the more modern LASIK (transmitting much less energy to the eye, and to the middle parts of the stroma, rather than to the framework) and SMILE. Here it is:
Corneal Transparency Evaluation
Department of Ophthalmology, Philipps University of Marburg, Marburg, Germany, doi: 10.3109 / 02713683.2015.1107590
58 eyes with myopia from 33 patients who underwent SMILE were compared with 58 eyes with 33 patients who underwent FS-LASIK. All procedures were performed using a VisuMax femtosecond laser and a MEL 80 excimer laser. The result was evaluated on 3 optically significant concentric radial zones (0-2 mm, 2-6 mm and 0-6 mm) around the apex of the cornea and on 3 different anatomical corneal layers (front, center and rear).
After SMILE overall, all layers of the cornea in the radial ring 0-6 mm showed no significant changes compared with the preoperative values. After FS-LASIK, the overall result was significantly reduced. Three months after the operation, the results evened out - there were no statistically significant differences between the two groups from all the annular spaces studied.
I translate the result: cloudiness with SMILE does not remain immediately, and cloudiness with femtoLASIK-methods almost completely disappear in 3 months.
My comment: by the way, the Hazes after PRK are visible decades later - as are the marks from the scars after keratotomy. Look like this:

Haze after PRK

Corneal scars after radial keratotomy
It is not yet possible to predict corneal tendency to hayz: the effect arises from the fact that the outer epithelium of the eye from the cells of the ectoderm (cornea) embryo separates the Bowman's membrane. When it is burned off with PRK, then a pseudoboumen's membrane is seen in histology - this epithelium is in direct contact with the ectoderm and begins to form a skeleton to replace the lost membrane. Not always this frame is transparent.
Bowman's membrane and Haze - the danger of PRK (transFRK)
PRK (transFRK, etc.) is a cheap practical and well-studied method. But it went from him to femtoLASIK-methods, and then to SMILE. Why? Now I will try to explain it in simple words, and then I will show the research.
In its morphology, the cornea as a pie consists of 5 layers: epithelium, anterior border (Bowman) shell, its own substance (stroma), posterior border (Descemet) shell and endothelium.
At the stage of embryonic development, three different types of tissue are formed: the epithelium develops from the surface ectoderm, the middle layer of the stroma from the mesoderm, and the internal layer of the endothelium from the neuroectoderm. As they develop and differentiate, each of these tissues needs isolation in order to preserve its structure and specificity, which is achieved by the development of borderline membranes parallel with them - the endothelium forms the Descemet's membrane, and the stroma - the Bowman's membrane.
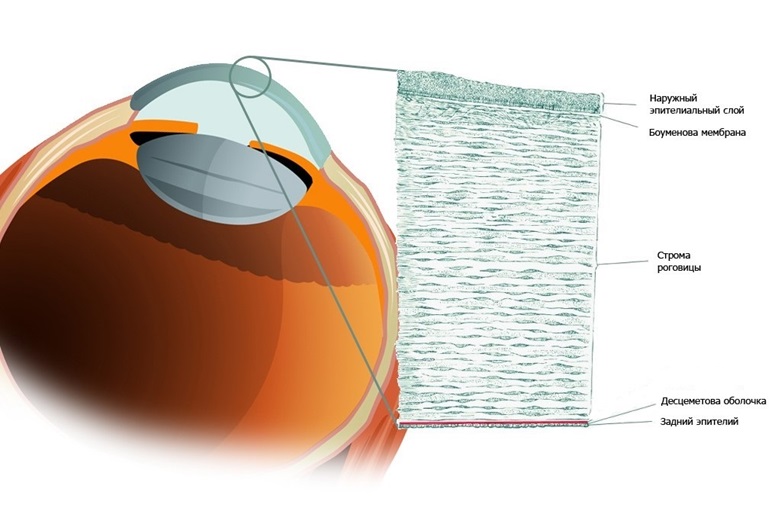
This is the structure of the cornea.
Normally, the cornea has physiological defects of the Bowman's membrane, through which nerve fibers penetrate the epithelium from the stroma. In a healthy cornea, there are few such openings, and there are certain protective mechanisms. When we evaporate the Bowman's membrane in PRK, we break down the protective barriers and cause inflammation, the body reacts to this by the formation of fibrous connective tissue. Just subepithelial and intraepithelial fibrosis is haze (haze (fleur) - from the English. Haze - fog). It is the reason for the rather slow achievement of the final results when performing photorefractive keratectomy (PRK), this remains one of the main problems of the method. The stabilization of refraction, as a rule, lasts several months and may be accompanied by regression or the occurrence of heyz.
Poorly treatable, marked turbidity, occur infrequently. But even a transient moderate haze during its existence can reduce the uncorrected sharpness and contrast of vision, which becomes a partial return to preoperative refraction and worsens the quality of life of patients.
Thus, the possible corneal opacification, the slow achievement of the optical effect and pain syndrome, make PRK (transFRC) one of the most unpopular methods of laser vision correction.
Traditional treatment after PRK involves the long-term use of corticosteroids, which allows to reduce the frequency and intensity of Hayes, as well as to some extent affect the postoperative dynamics of refraction. However, in some cases, corneal opacities in the photo-ablation zone are quite persistent and intense, which requires a different approach to treatment. In this case, laser and even surgical methods can be added to drug therapy.
It should be noted that when using PRK as a method of completing correction, the risks are minimal, since the refractive component to be corrected is small. Especially in combination with surface treatment with antimetabolites. But with the primary correction of more than 1-2 diopters, all the shortcomings of the PRK are manifested with might and main.
Here are the details about the complications.
Nerves recover, but it takes time. Therefore, after PRK-methods, supportive therapy is needed (up to six months) so that nothing bad happens to the eye during this time. Complete regeneration is enough to manage the trophic level takes about a year. In the SMILE method, only about 10-15% of the nerve endings are suppressed, which gives rise to significant differences.
The second feature is the cornea framework. The link is a description of keratoconus - protrusion of the cornea forward due to intraocular pressure. This is the most common complication, and it is extremely unpleasant. The only way to avoid it is to go deeper into the cornea. The cornea is heterogeneous. On the surface of the most durable layers. At a depth of 120 to 150 microns, loose layers begin. It is there that work is carried out on all methods starting with LASIK. With PRK we remove the strongest upper part of the stroma - see the picture above.
About the features of the fact that the epithelium and the stroma are best kept separated, I have already said. With PRK, this is not possible; with other methods, this is done.
Aberration
“Comparison of the visual results after SMILE and femtosecond laser-assisted LASIK for myopia. Lin F, Xu Y, Yang Y. "
Sixty eyes from 31 patients with an average spherical equivalent of –5.13 ± 1.75 diopters were subjected to myopia correction using the SMILE procedure. Fifty-one eyes of 27 patients with an average spherical equivalent of -5.58 ± 2.41 diopters were treated using the FS-LASIK procedure. Results: Neither 1 nor 3 months later, there were no statistically significant differences in visual acuity parameters. High order aberrations and spherical aberrations were significantly lower in the SMILE group than the FS-LASIK group.
Conclusion: SMILE has a lower level of higher order aberrations and a lower spherical aberration than the FS-LASIK procedure.
My comment: Visual acuity after femtosecond LASIK and after SMILE was quantitatively the same in two groups, but the quality of vision in the group after SMILE was higher due to smaller induced aberrations.
This is due, firstly, to the fact that the SMILE profile itself is aspherical, and creating such a profile with an excimer is possible only on modern machines and requires 5-10% more volume of cornea evaporation.
Secondly, the optical zone after SMILE is always slightly greater than or equal to the planned one, and for femtosecond LASIK it is slightly less than the planned one.
The damage factor, which is significant in femto and mechanical LASIK + + excimer laser effects are completely absent in SMILE.
Comparison of biological indicators of corneal damage
According to the study "Comparison of Corneal Biological Healing After Femtosecond LASIK and Small Incision Lenticule Extraction Procedure" (doi: 10.3928 / 1081597X-20140320-03) on 128 eyes (69 for SMILE, 59 for femtoLASIK). Tests were performed for visual acuity, refraction, a Norn test, a Schirmer test, a corneal sensitivity test, an ocular surface index, corneal hysteresis, and a cornea stability factor were measured. Measurements were taken before the operation, on the first day, a week, a month, a quarter and six months after the operation. Result - there was no significant difference in the results for vision for SMILE and femtoLASIK. After the operation in the femtoLASIK group, the sensitivity of the cornea was significantly reduced, slightly changed in the SMILE group. Biological corneal healing after SMILE surgery in the early period was superior to femtoLASIK.
My comment: in patients after SMILE, dry eye syndrome is much less pronounced, the sensitivity of the cornea and its strength are maintained at comparable postoperative visual acuity.

Schirmer test (for tear production) and its result

Norn's test (stability of the tear film)
Now the next study.
Biomechanical properties of the human cornea
doi: 10.1007 / s10792-017-0575-6
In this experimental study, 11 pairs of human corneas unsuitable for transplantation were divided into two groups. The corneas of the right eye were treated with a femtosecond laser LASIK (FSLASIK), the corneas of the left eye were treated with a small-length extraction of lenticles (SMILE). Pachymetry was measured in each eye immediately before the laser refractive surgery. All corneas were subjected to refractive correction of a sphere of -10.00 D and -0.75 D of a cylinder at 0 ° with a 7-millimeter area, either with a 110 μm flap (FS-LASIK), or with a 130-μm cap (SMILE). For two-dimensional biomechanical measurements, corneoscleral discs were subjected to two test cycles (a preliminary curve of strain dependence from 0.03 to 9.0 N and stress relaxation at 9.0 N for 120 seconds) to analyze the properties of an elastic and viscoelastic material. An effective modulus of elasticity was calculated. Statistical analysis was performed with a confidence interval of 95%.
When measuring strain-stress, the effective modulus of elasticity was 1.47 times higher. The size of the effect is significant. No significant differences were observed among relaxation-stress measurements with an average remaining voltage of 181 ± 31 kPa after SMILE and 177 ± 26 kPa and after FS-LASIK after relaxation.
Conclusions: compared with the flap-based procedure, such as FS-LASIK, the SMILE technique can be considered superior in terms of biomechanical stability, with experimental measurements on ex vivo paired human eyes.
My comment : before that, the same results were calculated by the method of mathematical modeling by Professor Ranstein (Great Britain), and Professor Sekundo confirmed the theoretical conclusions by measuring on paired human eyes (his cornea strength indicators after SMILE are even higher than in theory) in a special Swiss laboratory. These are truly revolutionary results!
So,
So what's better with myopia?
Let's go through the theses again:
- The operations of PRK, femtoLASIK and SMILE are neither better nor worse than each other, each has its own scope. PRK is logical to use as a method of correction, and for special medical purposes. For the primary correction should not be considered. FemtoLASIK can be done if there is no technological or financial ability to make SMILE, and the thickness and shape of the cornea can cut off the cover. ReLEx SMILE is the most sparing operation, the operation of choice with myopia and / or myopic astigmatism. It combines the advantages of two predecessor technologies, FemtoLASIK and PRK, but is devoid of their disadvantages.
- The PRK-method (trans-PRK) destroys the outer epithelium of the eye, the bowman membrane and the upper (most durable) layers of the cornea. In the minuses - a violation of innervation (and dry eyes), turbidity during the formation of pseudoboumenovoy membrane, the average risks of keratoectasia (corneal protrusion). In the pros - the ability to carry out this operation several times. PRK is certified in many countries for active sports.
In short, cool for those who love oldstyle-technology - ready to change the new Mercedes to the old Volga GAZ-21. - FemtoLASIK suppresses about 75-90% of the surface nerve endings in the cornea, the rest is barely enough to manage the trophism, but this is better than burning the entire surface. The work is going on in the loose layers of the cornea, the frame suffers because of the cut off of the cap. Due to the risk of displacement or separation, the flap is not allowed for correction in a number of dangerous professions and for athletes. If everything went smoothly, it gives a good optical effect and an accurate correction.
- SMILE - the most modern method, clinical use for more than 10 years: the first patients (with the exception of test pigs) have been walking after the operation since 2007. The cornea framework will remain, about 80% of nerves remain. It requires a unique VisuMax laser and a well-trained surgeon to extract the cut material through a narrow tunnel. The most painless operation that allows you to use your eyes from the next day without restrictions - this causes its cost. It gives the least amount of vision distortion due to aberrations. About two million operations around the world have now been performed, but the number of devices, clinics and operated patients is growing exponentially.
- Laser methods of vision correction are not the only possible methods of surgical vision correction: you can embed lenses in the eye, segments in the cornea, or replace your own lens with an artificial lens with new optical properties (more here ).
- Vision correction - in most cases is done because of the desire to improve the quality of life, rarely for medical reasons. Insurance medicine in most countries (including Russia) does not cover the costs of its implementation. It is up to you to make a vision correction or wear glasses / contact lenses, but in any case, to choose the right option you need to be information-savvy.
I suggest you decide, using the facts.
Source: https://habr.com/ru/post/423149/
All Articles