How to calculate the crazy: pathopsychological diagnosis
Hi, Geektimes! I am writing this post in collaboration with hdablin in the wake of his publication “Cognitive stimulants and another psychopharma: is it possible to become smarter,” devoted to the pharmacological aspects of the problem of “dispersal” of thinking. In it I want to talk about pathopsychology, about how people are tested for adequacy in a psychiatric hospital, about what violations of thinking are, how they are revealed, about where the difference between a geek and a mentally ill person passes, about whether diagnose a mental illness in oneself, and about many other things relevant to the subject.
About me: my name is Christina, I’m a medical psychologist (it’s a medical psychologist who graduated from a medical university with a degree in Clinical Psychology, this is important), she worked in a psychiatric hospital for three years, now she’s gone into private practice, but remained in psychiatry as in the industry . I have a specialization in neuropsychology. During my work I had to deal with various categories of patients - schizophrenics, BARschiki, depressive, organics; some of them applied voluntarily, some were hospitalized in an acute condition, some were “coercive” in general (these are people who committed a crime, but sent by the court not to prison, but to an insane asylum for compulsory treatment).
tl; dr : The article describes how, why and why the diagnosis of mental disorders is carried out.
I am aware of the fact that the general public often perceives psychology as a kind of “humanitarian boltological mud”, and I must say that this is not without reason. Sometimes, looking at my “colleagues”, practicing “astropsychology”, various kinds of “laying on hands”, etc., I want to burn my diploma, just to have nothing in common with them.
')
But I can assure you: not all psychology is like that. There are quite a variety of psychology working within the framework of a strict approach [1], and many types of psychotherapy (in fact, psychologists use psychotherapeutic techniques, although they are not psychotherapists) / corrections have proven effectiveness [2,3,4,5,6,7 ].
I will tell on the example of my experience in the mental hospital. In some institutions, the details may be different, but the essence itself is invariant.
So let's go!
Before proceeding to the consideration of specific methods of pathopsychological diagnosis, let's understand a little bit what it is and why it is needed. In general, pathopsychological diagnostics is a set of techniques and methods that help a specialist to identify certain violations of human mental activity.
In a psychiatric hospital, the diagnosis is divided into two stages: one is performed by a psychiatrist and the other by a medical psychologist. Ideally, the results should coincide, which, in turn, in theory, provides greater objectivity in the diagnosis and the development of treatment strategies. In fact, everything is not so rosy, and often either the psychiatrist copies the decision of the medical psychologist, or the latter asks him what to write in the conclusion, but let's not talk about the sad realities of domestic psychiatry, but consider the situation as it should be.
The psychiatrist in his work uses a clinical conversation (this is the official method in medicine), on the basis of which he makes a diagnosis using ICD-10. What is the main feature of the ICD is that it has quite distinct and clear criteria for attributing the set of phenomena that we can observe in the patient's behavior to a certain nosological unit. Everything is very simple there: if N signs from M are performed, then the diagnosis is appropriate. If not, look for another one.
We (medical psychologists) use not only clinical conversation, but also other methods: structured interviews, personal questionnaires, projective tests, etc. We are more specialized than psychiatrists. On the one hand, this allows us to see more details in the patient's mental life, but, on the other, it does not allow us to make diagnoses (since we have much worse preparation in the context of somatic phenomena).
Instead of making diagnoses, we detect symptom complexes.
Or like this:
That is, in simple words, a symptom complex is such a set of interrelated and mutually determined distortions in the work of the psyche that develops and exists as a whole.
The space of symptom complexes is non-linearly displayed on the space of diagnoses according to ICD-10. For example, a schizophrenic symptom complex can occur in people with a diagnosis of schizophrenia (F.20), schizotypical disorder (F21.8), schizoaffective disorder (F25.0).
Allocation of the symptom complex is useful, firstly, to control the main diagnosis (if the psychiatrist puts the patient on schizophrenia and the pathopsychologist sees an affective-endogenous symptom complex, then one of them is mistaken. It is necessary to double-check, use other diagnostic methods and understand in general).
Secondly, the choice of a symptom complex is already an interpretation. In the process of collecting raw data, we have at our disposal a sufficiently large number of parameters (both qualitative and quantitative), by which we can monitor the dynamics of treatment. Imagine: a chronic schizophrenic goes to hospital with an F.20 diagnosis. He leaves the hospital with the same diagnosis. But does this mean that nothing has changed?
If the hospital works normally (which is not always the case), then, of course, does not mean: the “before” condition can be characterized by the presence of productive symptoms (nonsense, hallucinations), and the “after” state can be a good compensation and social adaptation. And so, in order to assess these changes quantitatively and qualitatively, a repeated pathopsychological study is carried out. And within the framework of the same diagnosis, the patient will receive two different pathopsychological conclusions.
Thus, the results of pathopsychological diagnostics are useful during the entire period of treatment (and even after its termination - during screening): first, they are used to check and clarify the diagnosis, then they are used as one of the basis components for prescribing drugs and non-drug therapy (psychotherapy). , occupational therapy, art therapy, etc.), and then - to assess the success (or failure) of treatment.
Now, when we have approximately determined why pathopsychological diagnostics is carried out, let us consider in more detail the subject of the study itself.
One of the main stages of pathopsychological diagnosis is the study of the patient's personal characteristics. First of all, we define the personality radical (i.e., we make the characterological classification of the personality).
There are quite a few definitions of character [10], starting with the classic Freudian explanation of the personality on the basis of fixations and ending with the modern developments of ego psychologists, who emphasize defenses.
In my clinical work, I use the following empirically derived definition: a characterological type (or personality radical) is a stable, interconnected and interdependent set of ways that a person reacts, as well as ways of internal organization of mental processes.
There are many types of character: schizoid, hysteroid, obsessive-compulsive, narcissistic, depressive and others. Do not be misled by the apparent similarity of these names with terms and diagnoses and ICD. For example, schizoid does not necessarily suffer from schizophrenia or even schizoid disorder, and a depressed person is not necessarily depressed. Moreover, each can be attributed to one or another characterological type, and this type, most likely, will have a “offensive” name for a layman.
The relationship between type of character and mental disorders is complex and non-linear. Not only can schizoid not have schizophrenia, it can also have obsessive compulsive disorder or depression. Or a combination of both disorders.
It can be said [11] that (very much simpler!), Those signs that normally make up the characterological peculiarity of a person, the basis of his individuality, become aggravated in the disease and become hypertrophied. Thus, for example, schizoid profanity, imaginative and rich speech in schizophrenia degenerates into schizophasia. But the "roots", "beginnings" of this schizophasia can be traced in schizoid speech.
So, we classify our patients by type of character. This makes it possible, firstly, to approach them more effectively (for example, the schizoid should be approached from the standpoint of intellectual and logical reasoning, and the hysteroid will simply give a sense of understanding and human warmth).
Secondly, knowing the characterological type of the patient, we can more effectively select the strategies of psychotherapeutic and psychocorrectional effects. Third, we can more effectively predict the behavior of patients (for example, understand that the hysteroid is very likely to exaggerate the severity of their symptoms). The examples in this paragraph are deliberately exaggerated in order to show what it is in contrasts. Please do not take it as a guide to action.
For personality research, we use various kinds of projective tests, individual personal questionnaires, and countertransference analysis. I will tell about these methods below.
In this block, we explore, oddly enough, thinking. Or rather, looking for his violations. Or their absence (which can also be diagnostic, for example, by the absence of a slowdown in thought processes, it is possible to exclude the presence of serious endogenous depression).
The main types of disorders can be described as follows: a violation of the operational side of thinking, a violation of the motivational component of thinking, a disorder of the categorical structure of thinking, a decrease in the level of generalization.
The patient may be impaired ability to highlight the main and secondary. And to the question “what’s important in a car”, he will answer “that he is white” or “that I went with my father in a car for fishing”.
Excessive generalizations are possible when the patient is not able to isolate differences at all from different groups of objects, and in perception everything merges into one continuous mess.
Slippage is possible, in which patients, correctly solving a task or reasoning about an object adequately, patients unexpectedly stray from the correct train of thought due to a false association that has arisen, and then are able to continue the reasoning consistently, without correcting the error [12 ].
Reasoning is also a violation of thinking - the tendency of patients to fall into long, unrelated to the subject of reasoning, for example: “I once went to the store, by the way, and you know that the doors in the stores are made of iron, and we mined iron when I served in the army in the Urals, so service in the army is generally a mockery of a person: how can a boy be taken and taken away for two years, etc. ”(the example is fictitious).
There are also motivational-related violations of thinking, which manifest themselves in violation of the hierarchy of needs: if you exaggerate, when a tiger chases a patient, he does not think about how to be saved, but about how Nietzsche's philosophy influenced the development of the Bolshevik party.
There are still violations of the substantive side of thinking - the ideas of relationships (“they are watching me”), nonsense (“I am the illegitimate son of Putin and Merkel, I must own the world”), etc.
To diagnose and assess the degree of disturbed thinking, we use a number of standardized and non-standardized methods for assessing thinking [13], analyzing patient's speech, structured interviews, and clinical conversation.
Everything is simple: there are several types of memory (even not so, there are many ways to classify memory, within each of which there are several types). And almost every one of them we can explore.
In practical work, I share the study of direct memorization (when we ask the subject to memorize something, and then, after a while, to reproduce) and indirect memorization.
In the first case, the standard “de facto” is the method of “Ten words” [14], in which the subject is read ten short unrelated words five times in a row, and after each time he is asked to play them in a random order. Long-term memory is tested by interviewing the subject in an hour.
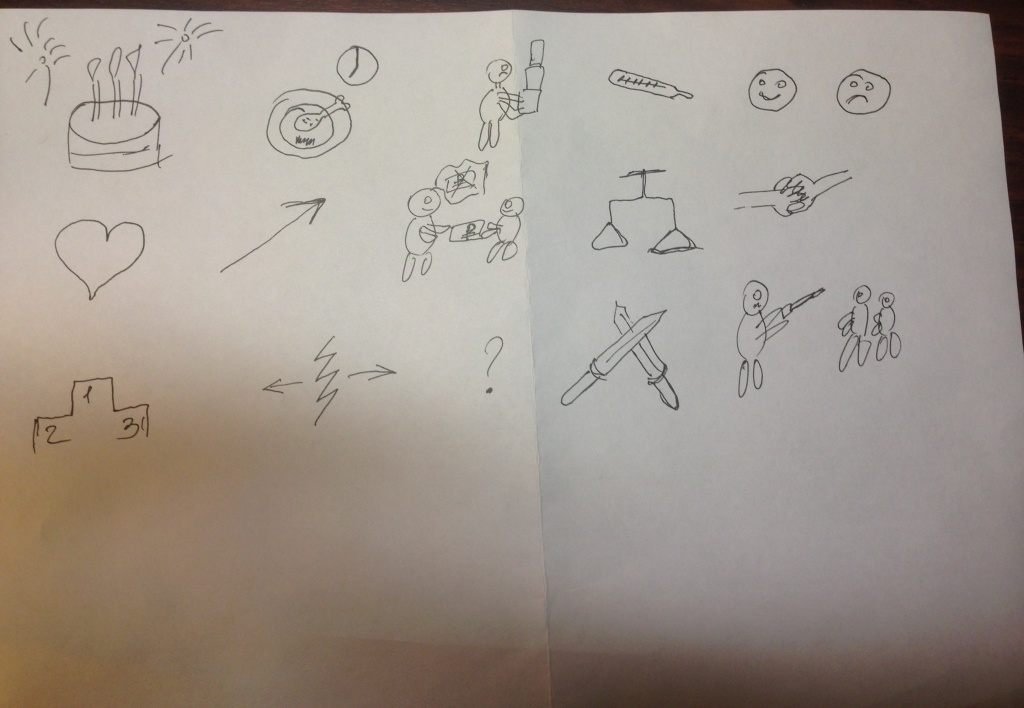
Indirect memorization is called so because the subject is allowed to use associations to facilitate memorization: for example, to draw pictures that will display an image that allows you to better remember the named word or phrase (for cheaters: you cannot sign).
The trick of the methods of the study of mediated memorization is that, besides, in fact, memory, they very well allow you to explore the mindset (see the previous section) [14]. Below I will show an example.
The fact that such intelligence, fierce battles, which are still very far from complete. Personally, I like to use so-called in work. Spearman's G-factor [15] is a value that characterizes the “general intelligence factor”, which is culturally independent and is verified by non-verbal methods. But here the preferences are explained not so much by theoretical views as by the presence of extremely convenient tools - Raven's progressive matrices (which we will discuss below), which can show an adequate assessment of the intellectual abilities of people with different education, cultural background, etc.
As an additional tool, I sometimes use the Wechsler test [16]. The results of this test already depend on the level of education and training of the subject, so by comparing the results of these two tests, we can determine, for example, the degree of pedagogical neglect (when the result is high for Raven and low for Wexler).
Intellect we measure, firstly, to make a diagnosis of mental retardation, secondly, to assess the severity of organic injuries, if any, and, thirdly, to assess intellectual disabilities in schizophrenia. In addition, the strategy of psychotherapeutic or psychocorrectional work with him (some are not able to understand the interpretations given by the psychotherapist) depends on the level of intellect of the subject.
In addition to general intelligence, we also measure social and emotional intelligence. The first is, in simple terms, the ability to correctly understand the behavior of other people. The second is the same, but about emotions.
Indicators on these criteria are important for determining the degree and nature of impaired mental processes, especially in schizophrenia with its emotional-volitional defect.
For the study of social intelligence, I use the test of Guilford, and for emotional - test TAT.
Attention is the ability of purposeful concentration of perception [17], and it also is impaired. It can independently, besides the will of the test subject, “jump from object to object,” can be depleted, etc.
In general, as a rule, a qualitative assessment of attention can be given simply on the basis of observation of the patient during a clinical conversation and subsequent pathopsychological research. But if I need a quantitative assessment, I use the Schulte tables, the Crepelin score, the Münsberger test, etc.
Attention we appreciate in order to assess the degree of organic disorders, the power of volitional decline in schizophrenia, to identify manic and depressive phases in BAR (as an auxiliary method).
And with these tests it's cool to keep track of the side effects from neuroleptics, trunks and mood stabilizers.
Mental status is a characteristic of the patient's current psychoemotional state, i.e. how he feels, what he experiences, how he realizes, where he is, who he is, and why he is there.
We assess our mental status mainly by observation (it is believed that a good specialist can make a diagnosis while the patient passes the post from the door of his office to the chair) and clinical conversation.
Determining mental status, we find out such parameters as accessibility to productive contact (the patient is able to answer questions distinctly and on the topic), orientation in time (what's the date), space (where he is) and self (who is he, why was he ).
Knowledge of mental status allows us to determine the symptom complex, and doctors - to make a diagnosis. Again, with it you can track the dynamics of treatment.
Here we see how the patient is captured by emotions, what kind of emotions are - depression, joy, fear, etc., and also how much he is capable of volitional regulation, i.e. to purposeful continuous activity.
Again, personally, I usually use clinical conversation and observation here, but there are also instrumental assessment methods [18] - such as TAT [18].
But usually the need for instrumental measurements of the parameters of the emotional-volitional sphere does not arise.
We are interested in this area in the sense that information about it helps to identify the correct symptom complex, and repeated research allows us to more accurately track the dynamics of treatment.
So, after we have decided on what and why we are exploring, we can proceed to the most interesting part - the consideration of specific methods of pathopsychological research.
The SMIL test (standardized multifactor personality research questionnaire) is an adaptation to the domestic realities of the well-known western MMPI test [12]. It includes 566 questions (it takes from one and a half hours to complete), for each of which it is possible to give one of three answers: “yes”, “no”, “I don't know”.
Example of questions from SMIL:
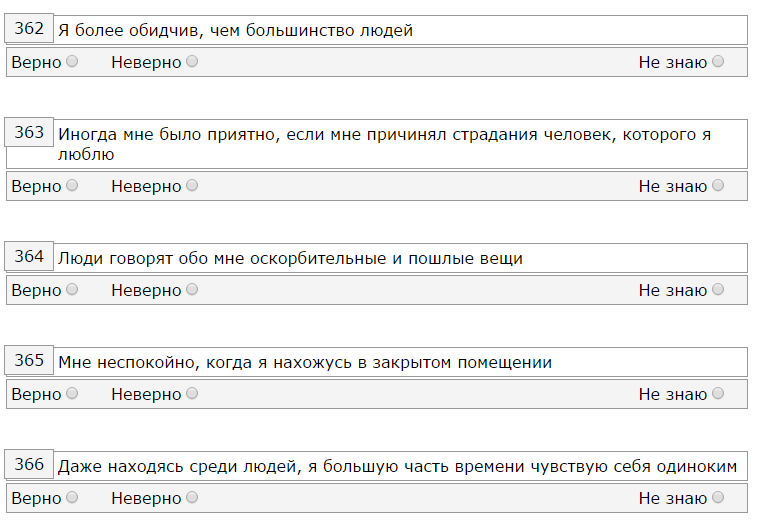
The questions are rather tricky: there are questions to check attentiveness, there are different reformulations of the same statement, there are antagonistic questions. The absolute majority of patients who are first passing SMIL cannot calculate the mechanism of its work, which plays into our hands.
As a result, we get the result in the form of graphs, which are convenient to use to track the effectiveness of treatment. Here is an example of the results of hdablin - the first picture after leaving the mental hospital:

... the second - after about 7-8 months of pharmaco-and psychotherapy in self-treatment mode:

I think it's time to talk about what these charts are, and what they mean. On the abscissa we have the scale. The first three are so-called. confidence scales. The next ten are the main scales.
On the first three scales, we can conclude about how sincere the subject was, whether he tried to put himself in a better or worse light. Sometimes (as in the presented example) it happens that the profile is unreliable formally, but it can be analyzed at the discretion of the interpreter (the gray zone is spelled out in the methodology. But even the patient tried to deceive us (consciously or unconsciously) is usually visible: if he frankly lied, the scale of L (scale of lies) will be increased, if he tried to speak against himself or was anxious - the scale of F (confidence), and if he tried to conform to a certain ideal image, then the scale of K (correction).
The basic information about the subject is given by scales from 1 to 0: Scale of supercontrol, pessimism, emotional lability, impulsivity, masculinity-femininity, rigidity, anxiety, individualism, optimism, introversion [12].
But earlier they were called much clearer: hypochondria, depression, hysteria, psychopathy, masculinity - femininity, paranoia, psychasthenia, schizophrenia, hypomania, social introversion. Agree, so much clearer?
How to interpret this test? Each scale is assigned certain properties. For example, the eighth scale is originality of thinking, the third scale is demonstrativeness, and the second is avoidance behavior.
Up to certain numerical values (65 points), these properties have the appearance of character traits, then - up to 75 - accentuations (this is when, in general, the peculiarity of living does not seem to interfere with living, but in some circumstances is destructive), and even further - this is pathology and perhaps even a mental illness.
Those. on the example of my favorite schizoids, to which I myself belong, 65 points on a scale of 8 - this is originality and singularity, but, here it is 80 on it, - this should be checked for schizophrenia.
According to SMIL, a lot of interesting things can be calculated - to determine the radical of a person, to understand how a person copes with difficulties, what to expect from him in an extreme situation, what kind of work suits him, what motivation prevails - achieving the goal or avoiding failure, etc.
For example, according to the second picture from the illustration above, we can say that the profile smoothed out, somewhat approaching the ideal one (the ideal unattainable profile is a straight line at 50 points), we see that the level of depression has decreased, which has decreased destructive impulsivity, which has decreased very much anxiety, and the characterological basis - a mixed schizo-hysteroid radical - has been preserved.
, , , MMPI HR- . : 2 7 3 4, , « » , , , . , « » , , , .
, . -, . , -. -, : , . -, , .
, ( ), 71 . . , , . .
. .
, , , . , : / . , . . , , .. , .
: , , , . . — , ..
, , - , , , , . : , , , , ..
, : , — . , , ( ) , .
«». « ».
: A4 . , ( , ).
, , , , . , . , , .
: a. , b. , c. , d. , e. , f. , g. , h. , i. , j. , k. , l. , m. , n. , o. , p. .
, , ( «») : . .
, hdablin , ( , , , ):
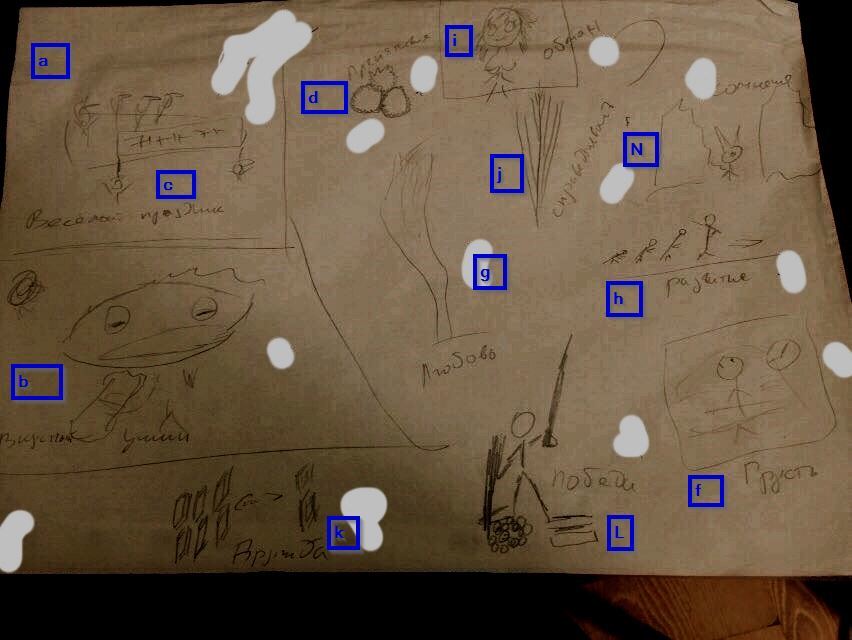
:
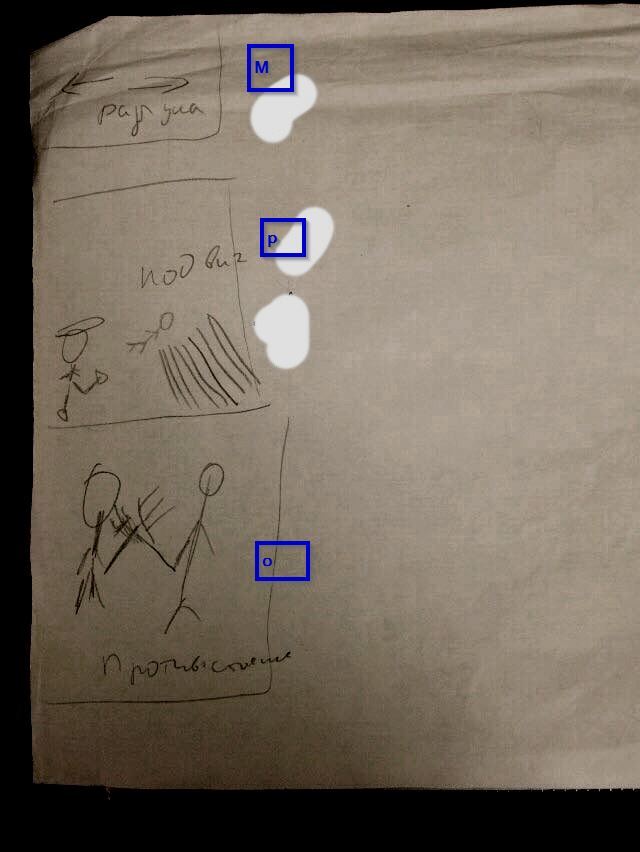
: «», («» «», ) , , . « », - . « » « » . , «» .
, [13] , . ? , : (.. ) , , .
. , , :
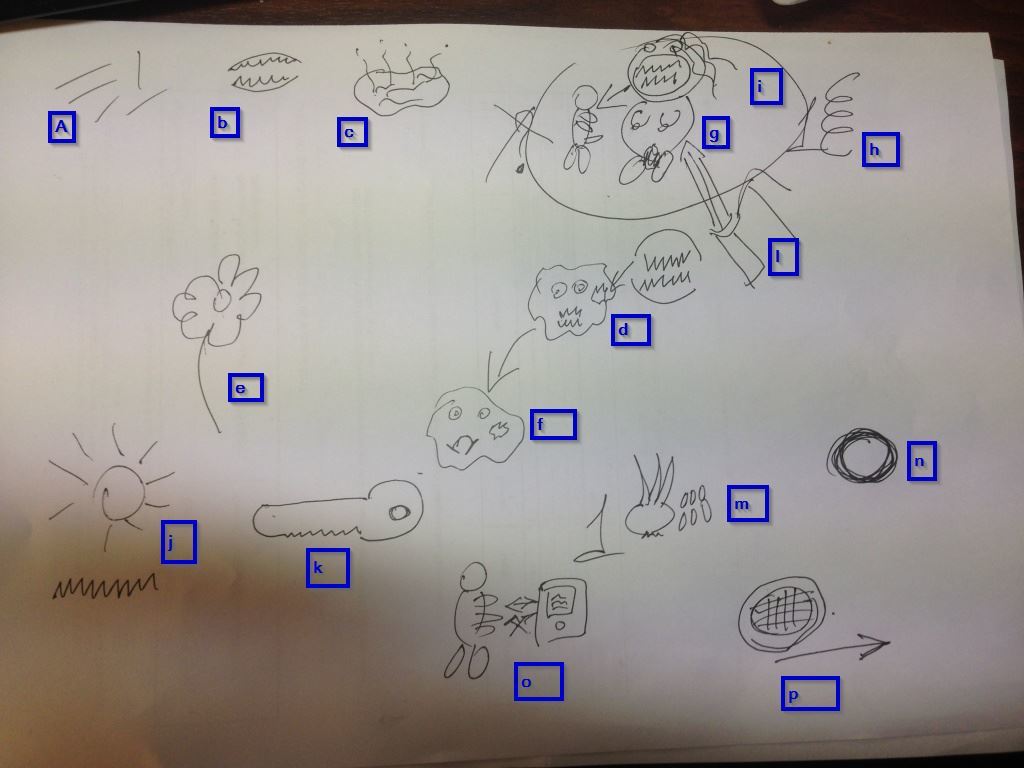
(). , , .
a) — «, , , »
b) — « , »
c) — «. , — »
d) — « . » ( )
e) — «. , , »
f) — « , »
g) — « »
h) — « » ( )
i) — « , »
j) — « , — »
k) — «» ()
l) — « »
m) — «, » ( )
n) — « »
o) — « »
p) — « » ( ).
, — :
, .
, , , . [13] :
a. , , ( — );
b. ;
c. ( ) ;
d. ;
e. ( )
Other.
, , .
. , , , ( ), . « , » , .
, [19]: , , , ..
, , , , , (, , - , , ).
, [19], . : , « — », «» . , , , .
, [19] , , -, , , -, , , ( — , , , , ).
, , , . , . , , ( ) . , , , , , : , , , , ( ).
« ». , , : , , .. Use pre-made fictional characters from works of art, mythology, religion, etc. - prohibited.
, , , : , . , , . , .
, , , — - , , .
, , , hdablin :
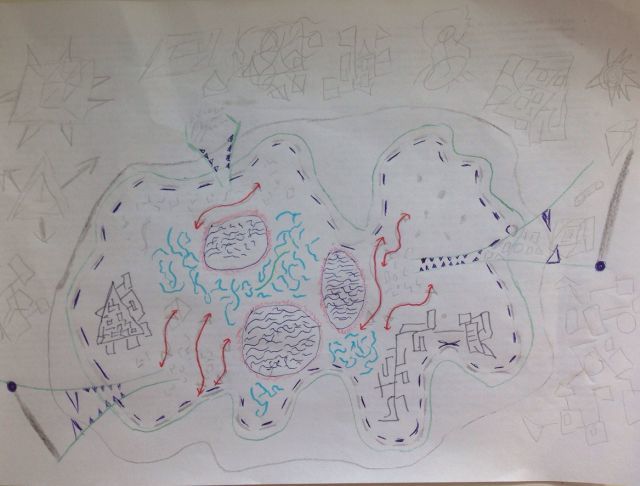
, , , , , , , ( , — ). , , .
— :
, , , ( , , ), , .
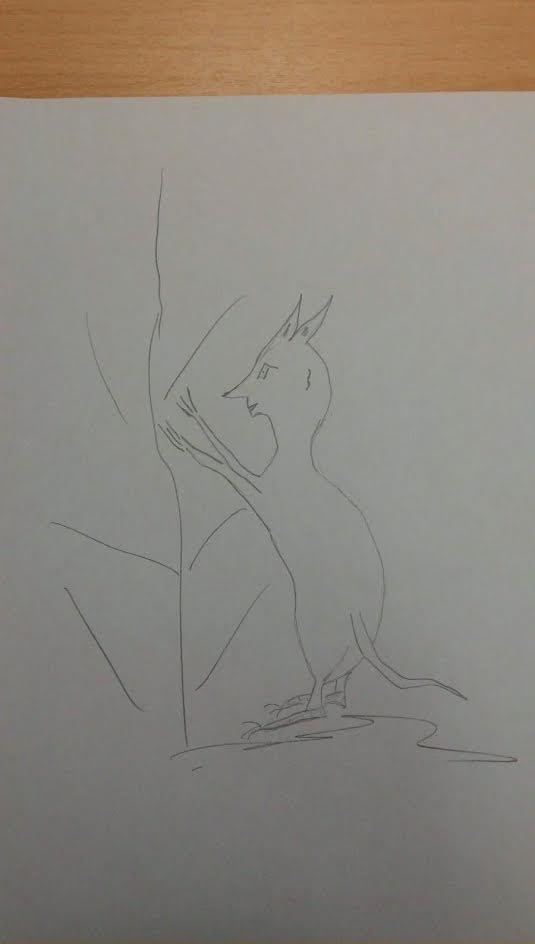
— ( hdablin ):
, , , , , , , , – . , — , ..
- , , . , «».
. , , ( ). , , .
( ) [20]:
:

A healthy person will come up with some plausible plot, without too elaborate details. The schizophrenic is very likely to confine himself to a formal description of the painting in the spirit of "two men cut the third, and the boy faces us."
, , .
Quite often it is necessary to test the attention of the patient. The easiest way to do this is by giving it load testing. For example, you can force him to look for numbers in Schulte's tables.
They are cards, which show tables of 5 x 5 cells. Each cell contains a number from 1 to 25 inclusive. Numbers are randomly distributed. The task of the subject is to indicate in turn all the numbers from 1 to 25 in the minimum time. This task is given to the subject five times in a row.
An example of such a table (there are all the necessary numbers, honestly!):
Observing how the subject performs this task, you can collect quite a lot of information about him: the pace of thinking (accelerated, normal, slow), assess the concentration of attention, its stability, exhaustion, type of response, etc. Normally, searching all numbers should take 40-50 seconds.
We need quantitative indicators of intellect for making diagnoses (especially for determining the gradations of mental retardation), for determining the degree of development of a schizophrenic defect, etc.
Personally, I use Raven progressive matrices for this purpose. Their trick is that they measure intelligence precisely as the ability to find solutions, and not as having some kind of knowledge, training in certain areas, etc.
The essence of the test is very simple: you need to select a picture to the sequence. For example, like this:
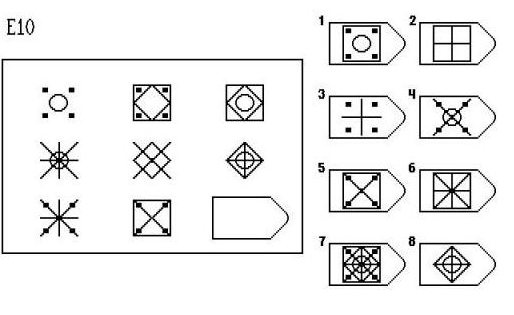
Again, besides, in fact, the level of intelligence, you can assess a bunch of other factors: attention, fatigue, composure :)
This test shows the ability to understand and predict the behavior of other people. Quite often it happens that the intellect (which is in the previous section) is preserved and even high, and social intelligence is “like a stool” (a characteristic that his psychotherapist gave to hdablin).
The test consists of four categories, in three of which you need to select the appropriate picture. In the first part, you need to choose the end of the story, in the second part - a picture that expresses a certain state or a person’s feeling, in the third one, by the existing phrase, determine who and to whom it could be said and, finally, in the fourth part, select the missing picture to make a related story.
Example of pictures from the first part (here you need to select the following action):
This test quite well shows a person’s ability to recognize and use various social signals and helps in the diagnosis of schizophrenia and mental retardation.
Thinking can be investigated not only through indirect memories and associations, but also directly. A popular technique for this purpose is the “Classification of Objects” test. The subject is offered 71 cards containing images of various objects and the task to group them.
If the subject asks a question about exactly how to group them, they are answered evasively - “as you see fit,” “how do you think is right,” etc.
Cards look like this (in the picture there are four different cards, not one with four items):
A complete list of cards: sailor, baby dress, poppy flower, blacksmith, thermometer, beetle, scissors, swallow, cart, horse, inkwell, watermelon, bicycle, boletus, bow, plane, notebook, doctor, truck, globe, pocket watch, cherry, cup and saucer, sofa, boots, fox, dog, table, goldfish, dog, pan, lamb, bed, centimeter, pigeon, pig, saw, shtangeltsirkul, swan, pine, beetroot, pear, bottle, bookcase, carrot , broom, deciduous tree, cleaning lady, glass, mushroom amanita, cat, books, dipper, fur cap, goat, scales, butterfly, ka RP, goose, apple, wardrobe, child, jacket, elephant, lily of the valley, rooster, bear, skier, motor ship, plum.
Healthy people from these items usually collect the following groups: people, measuring devices, school equipment, kitchen utensils, vehicles, clothing, furniture, vegetables, mushrooms, fruits, flowers, animals, birds, tools, household items.
Patients often create very bizarre associations, for example, a cleaning woman, a wardrobe, a table and a cart are combined on the basis of the presence of something wooden in these images; or table, whatnot, cat, dog and horse - because they have four legs, etc.
So, we have reviewed the main groups of tests that can be used when conducting pathopsychological research. Now it is necessary to tell a little about how their results agree with each other.
The beginning of the examination occurs when the specialist sees the patient (when the latter enters the office). It uses the observation method. An experienced psychologist can make some assumptions about the subject by the first seconds of contact, and he makes them.
Further, anamnesis is collected (aha, again, it is collected twice - by a psychiatrist and a psychologist) and a clinical conversation.
In principle, it may be enough for a good specialist to reasonably expose a certain symptom complex, but instrumental testing is carried out to control and exclude subjective factors.
At this stage, the psychologist already has a certain model of the subject's mind, and is trying to confirm, refute or clarify it. He can conduct a structured interview (it differs from a clinical conversation by having a hard list of questions and a scoring system for evaluating answers to them), after which this model is further refined.
Further, when conducting instrumental testing, there may be evidence in favor of the existing hypothesis regarding the device of the subject's psyche, or its denial. In the latter case, the specialist is required to find an explanation for the discrepancies and include this explanation in the next version of the model.
In general, the essence comes down to the fact that the final positions that will form the basis of the choice of a symptom complex are constantly checked both for logical compatibility between each other and by using different methods.
If, for example, in a SMILER, a test subject has low values on a scale of 3 (emotional lability), and his non-existent animal has a huge peacock tail, eyelashes, and all kinds of curls (a sign of demonstrativeness that should have appeared on a scale 3), then something wrong here.
And then it is necessary either to recognize the unreliable result of SMIL (sometimes the validity scales do not show anything, leaving the decision on the validity or invalid profile at the discretion of the interpreter), or understand that these curls are not curls at all, but some organs, and the tail from possible values (not as a demonstrative, but as a significance of the sexual sphere), or to examine the subject for simulations / dissimulations.
Yes, in pathopsychology there are no such strict and quantitatively definite diagnostic methods, as, for example, in endocrinology, but constant cross-checks allow achieving quite acceptable accuracy.
The World Health Organization identifies the following mental health criteria:
• awareness and sense of continuity, constancy and identity of one’s physical and mental “I”.
• a sense of constancy and identity of experiences in situations of the same type.
• criticality to oneself and one’s own mental production (activity) and its results.
• correspondence of mental reactions (adequacy) to the strength and frequency of environmental influences, social circumstances and situations.
• the ability of self-management behavior in accordance with social norms, rules, laws.
• the ability to plan their own livelihoods and implement these plans.
• the ability to change the way of behavior depending on the change of life situations and circumstances [22].
In principle, I agree with these criteria. But the main thing, in my opinion, is the ability of a person to live without bringing excessive unreasonable difficulties to himself or others. That is why I believe that a happy compensated (that is, a schizophrenic who has found his place in life and firmly established in him) is healthier than a hapless neurotic.
And yes, not always and not all oddities are necessarily a symptom of a mental illness. They can be useful in diagnosis, just as a source of information, but if, for example, you live in central Russia, but all your girls are African, then this is not a reason to consider you sick. Modern psychiatry allows a fairly high degree of variation in behavior.
One of the most frequently asked questions to me is whether it is possible to deceive a diagnostician. There is no definite answer to it. It depends, as they say.
If the subject knows the subject (pathopsychology and psychiatry) is much better than a psychologist and a doctor, then, theoretically, yes, he can simulate or dissimulate. It is very difficult: you need to constantly remember about a huge number of factors, one incorrectly set line in the pictograms can completely destroy the image formed by the cheater.
In addition to good knowledge in the subject area, you need to have a very good body control and be a good actor, otherwise it will be seen from nonverbalism that “something is not right here,” and no perfect pictogram will help.
And we sometimes openly provoke our subjects, and they can break under the pressure of emotions, discovering their true nature.
Well, the most difficult thing is pills. In our hospital, the patient cannot but receive medical treatment. He must be given pills, but they don’t say which ones, he doesn’t know which drugs are prescribed for him. And if he wants to deceive someone, he will have to be very hard: you need to understand what these drugs are and how they would affect the person he is portraying.
On the other hand, our hypothetical deceiver is not alone in the department; he may well find a person of the type who depicts, among patients, visually compare the tablets and injections received, and using his observation skills, identify some of the changes that have appeared in the “donor of behavior” since prescription drugs, and copy them. But this is already from the realm of fantasy, for which our psychiatrists could examine me myself :)
Yes, one more thing: one often encounters the fact that someone tries to somehow offend or shock a psychologist, for example, by drawing a genital organ, excrement, and something like that. So, the trick is that, firstly, such an act is itself diagnostic, and, secondly, how this object is drawn can give exactly the same information that could be obtained from an honestly executed drawing .
The last question I would like to consider is the possibility of self-diagnosis. Let's do this: it is impossible to diagnose a severe mental disorder in oneself. Just because such disorders significantly distort perceptions of reality, and if you begin to see aliens, then most likely you will have some explanation for this (the literature describes cases of critical attitudes even to the first hallucinations, but this is rare).
For a depressed patient who is on a psychotic level, it seems that he is just objectively bad, and he is genuinely surprised by the stupidity of others who do not understand this, the patient in a manic state sincerely believes that he is such an awesome person, so you can sell an apartment, take a bag loans and arranging a farm for breeding sepules (and it doesn’t matter that no one saw them, they, the others, are simply not good enough for such an activity), an avid PCR specialist can give you a link to clinical studies that “will confirm his need to constantly wash hands, etc.
And the point here is not that a person has no potential knowledge. Even an experienced psychiatrist / medical psychologist cannot self-diagnose himself (in general). Just because the disease creates in our perception "blind spots" that do not allow it to be detected.
However, something a person can do himself. First, he can turn to a specialist as soon as he feels that something is wrong with him. Secondly, to some extent it can withstand light neuroses [21]. Thirdly, he may ask someone to take him to a specialist (for many it is important).
I hope the article fits into the theme of the resource and will find its reader. If you like it, I will try to write the same, but about neuro-and not pathopsychology.
You can ask any questions in the comments, but keep in mind that, firstly, it is impossible to identify a symptom complex (I do not make diagnoses) by commenting, and, secondly, some information from the discharge “but how was it in your mental hospital?” I didn’t I can cite for ethical reasons.
1. ru.wikipedia.org/wiki/Experimental_psychology
2. Cochrane evidence. Psychological therapies for pathological and problem gambling.
www.cochrane.org/CD008937/DEPRESSN_psychological-therapies-for-pathological-and-problem-gambling
3. Cochrane evidence. Cognitive behavioral therapy for people with asthma. www.cochrane.org/CD011818/AIRWAYS_cognitive-behavioural-therapy-people-asthma
4. Cochrabe evidence. Psychosocial and psychological interventions for postpartum depression.
www.cochrane.org/CD006116/DEPRESSN_psychosocial-and-psychological-interventions-for-postpartum-depression
5. Otte C. Cognitive behavioral therapy in anxiety disorders: current state of the evidence. Dialogues Clin Neurosci. 2011; 13 (4): 413-21.
www.ncbi.nlm.nih.gov/pubmed/22275847
6. Emma Robinson, Nickolai Titov, Gavin Andrews, Karen McIntyre, Genevieve Schwencke, and Karen Solley. Internet Treatment for Generalized Anxiety Disorder: A Randomized Controlled Trial Comparing Clinician vs. Technician Assistance.
www.ncbi.nlm.nih.gov/pmc/articles/PMC2880592
7. Foroushani PS, Schneider J, Assareh N. Meta-review of computerized CBT in treating depression.
www.ncbi.nlm.nih.gov/pubmed/21838902
8. Kudryavtsev, I.A. Comprehensive forensic psychological and psychiatric expertise (scientific and practical guidance). - M .: Publishing House of Moscow. University, 1999, p. 55
9. Medical psychology: Lecture notes / Comp. S.L. Solovyov. - M .: LLC "Publishing AST"; SPb .: Sova LLC, 2004, p. 28
10. N. McWilliams. "Psychoanalytic Diagnostics: Understanding the Personality Structure in the Clinical Process"
11. L.N. Sobchik. “Standardized multifactor method of personality research”
12. Schizophrenic syndrome // Medical psychology: Lecture notes / Compiled by S.L. Solovyov - M-SPb, 2004, p. 44-56
13. B.G. Kherson. “Clinical psychodiagnostics of thinking” - M.:, Meaning, 2014.
14. Rubinstein S. Ya. R 82 Experimental methods of pathopsychology. - M .: ZAO Publishing House EKSMO-Press, 1999. - 448 p. (Series "World of Psychology").
15. Cold MA - "The psychology of intelligence: the paradoxes of research."
16. Wechsler D. Manual for the Wechsler Adult Intelligence Scale. NY, 1955
17. Komarova T. K. Psychology of attention: Textbook.-method. allowance. - Grodno: GrSU, 2002. - 124 p.
18. Blacher V.M., Kruk I.V., Lateral S.N. Clinical Pathopsychology: A Guide for Physicians and Clinical Psychologists. - M .: Publishing House of the Moscow Psychological and Social Institute; Voronezh: Publishing house NPO “MODEK”, 2002.- 512 p. (Series "Library of the psychologist").
19. Wenger A.L. Psychological drawing tests: Illustrated manual. - M .: Vlados-Press, 2003. - 160 p: il.
20. Leontiev D.A. Thematic apperceptive test. 2nd ed., Stereotypical. M .: Meaning, 2000. - 254 s
21. Karen Horney. "Introspection"
22. Eliseev V.V. Psychosomatic diseases. Directory ... - Moscow, 2003.
About me: my name is Christina, I’m a medical psychologist (it’s a medical psychologist who graduated from a medical university with a degree in Clinical Psychology, this is important), she worked in a psychiatric hospital for three years, now she’s gone into private practice, but remained in psychiatry as in the industry . I have a specialization in neuropsychology. During my work I had to deal with various categories of patients - schizophrenics, BARschiki, depressive, organics; some of them applied voluntarily, some were hospitalized in an acute condition, some were “coercive” in general (these are people who committed a crime, but sent by the court not to prison, but to an insane asylum for compulsory treatment).
tl; dr : The article describes how, why and why the diagnosis of mental disorders is carried out.
I am aware of the fact that the general public often perceives psychology as a kind of “humanitarian boltological mud”, and I must say that this is not without reason. Sometimes, looking at my “colleagues”, practicing “astropsychology”, various kinds of “laying on hands”, etc., I want to burn my diploma, just to have nothing in common with them.
')
But I can assure you: not all psychology is like that. There are quite a variety of psychology working within the framework of a strict approach [1], and many types of psychotherapy (in fact, psychologists use psychotherapeutic techniques, although they are not psychotherapists) / corrections have proven effectiveness [2,3,4,5,6,7 ].
I will tell on the example of my experience in the mental hospital. In some institutions, the details may be different, but the essence itself is invariant.
So let's go!
A bit about pathopsychological diagnosis
Before proceeding to the consideration of specific methods of pathopsychological diagnosis, let's understand a little bit what it is and why it is needed. In general, pathopsychological diagnostics is a set of techniques and methods that help a specialist to identify certain violations of human mental activity.
In a psychiatric hospital, the diagnosis is divided into two stages: one is performed by a psychiatrist and the other by a medical psychologist. Ideally, the results should coincide, which, in turn, in theory, provides greater objectivity in the diagnosis and the development of treatment strategies. In fact, everything is not so rosy, and often either the psychiatrist copies the decision of the medical psychologist, or the latter asks him what to write in the conclusion, but let's not talk about the sad realities of domestic psychiatry, but consider the situation as it should be.
The psychiatrist in his work uses a clinical conversation (this is the official method in medicine), on the basis of which he makes a diagnosis using ICD-10. What is the main feature of the ICD is that it has quite distinct and clear criteria for attributing the set of phenomena that we can observe in the patient's behavior to a certain nosological unit. Everything is very simple there: if N signs from M are performed, then the diagnosis is appropriate. If not, look for another one.
We (medical psychologists) use not only clinical conversation, but also other methods: structured interviews, personal questionnaires, projective tests, etc. We are more specialized than psychiatrists. On the one hand, this allows us to see more details in the patient's mental life, but, on the other, it does not allow us to make diagnoses (since we have much worse preparation in the context of somatic phenomena).
Instead of making diagnoses, we detect symptom complexes.
The pathopsychological symptom complex is a relatively specific pattern (in a certain way organized complex, structured set) internally related, related by origin (pathogenesis) and development mechanisms of psychological phenomena (symptoms) - signs of behavioral disturbances, emotional response and cognitive activity, carrying information about the level (depth ), the amount (severity) of mental damage and some of its nosological characteristics (diagnostic "color") [8]
Or like this:
As in psychiatry, in pathopsychology, a syndrome is understood as a pathogenetically determined commonality of symptoms, signs of mental disorders, internally interdependent, interrelated. This is a great diagnostic significance of syndromes compared with symptoms. In the diagnostic thinking of the doctor, the correct qualification of the syndrome is an approach to determining the nosological origin of the disease. Each of the pathopsychological syndromes includes a number of symptoms. A set of symptoms is a syndrome (symptom complex). Syndrome - due to the general pathogenesis of a stable combination of interrelated positive and negative symptoms [9]
That is, in simple words, a symptom complex is such a set of interrelated and mutually determined distortions in the work of the psyche that develops and exists as a whole.
The space of symptom complexes is non-linearly displayed on the space of diagnoses according to ICD-10. For example, a schizophrenic symptom complex can occur in people with a diagnosis of schizophrenia (F.20), schizotypical disorder (F21.8), schizoaffective disorder (F25.0).
Allocation of the symptom complex is useful, firstly, to control the main diagnosis (if the psychiatrist puts the patient on schizophrenia and the pathopsychologist sees an affective-endogenous symptom complex, then one of them is mistaken. It is necessary to double-check, use other diagnostic methods and understand in general).
Secondly, the choice of a symptom complex is already an interpretation. In the process of collecting raw data, we have at our disposal a sufficiently large number of parameters (both qualitative and quantitative), by which we can monitor the dynamics of treatment. Imagine: a chronic schizophrenic goes to hospital with an F.20 diagnosis. He leaves the hospital with the same diagnosis. But does this mean that nothing has changed?
If the hospital works normally (which is not always the case), then, of course, does not mean: the “before” condition can be characterized by the presence of productive symptoms (nonsense, hallucinations), and the “after” state can be a good compensation and social adaptation. And so, in order to assess these changes quantitatively and qualitatively, a repeated pathopsychological study is carried out. And within the framework of the same diagnosis, the patient will receive two different pathopsychological conclusions.
Thus, the results of pathopsychological diagnostics are useful during the entire period of treatment (and even after its termination - during screening): first, they are used to check and clarify the diagnosis, then they are used as one of the basis components for prescribing drugs and non-drug therapy (psychotherapy). , occupational therapy, art therapy, etc.), and then - to assess the success (or failure) of treatment.
Now, when we have approximately determined why pathopsychological diagnostics is carried out, let us consider in more detail the subject of the study itself.
Personality research
One of the main stages of pathopsychological diagnosis is the study of the patient's personal characteristics. First of all, we define the personality radical (i.e., we make the characterological classification of the personality).
There are quite a few definitions of character [10], starting with the classic Freudian explanation of the personality on the basis of fixations and ending with the modern developments of ego psychologists, who emphasize defenses.
In my clinical work, I use the following empirically derived definition: a characterological type (or personality radical) is a stable, interconnected and interdependent set of ways that a person reacts, as well as ways of internal organization of mental processes.
There are many types of character: schizoid, hysteroid, obsessive-compulsive, narcissistic, depressive and others. Do not be misled by the apparent similarity of these names with terms and diagnoses and ICD. For example, schizoid does not necessarily suffer from schizophrenia or even schizoid disorder, and a depressed person is not necessarily depressed. Moreover, each can be attributed to one or another characterological type, and this type, most likely, will have a “offensive” name for a layman.
The relationship between type of character and mental disorders is complex and non-linear. Not only can schizoid not have schizophrenia, it can also have obsessive compulsive disorder or depression. Or a combination of both disorders.
It can be said [11] that (very much simpler!), Those signs that normally make up the characterological peculiarity of a person, the basis of his individuality, become aggravated in the disease and become hypertrophied. Thus, for example, schizoid profanity, imaginative and rich speech in schizophrenia degenerates into schizophasia. But the "roots", "beginnings" of this schizophasia can be traced in schizoid speech.
So, we classify our patients by type of character. This makes it possible, firstly, to approach them more effectively (for example, the schizoid should be approached from the standpoint of intellectual and logical reasoning, and the hysteroid will simply give a sense of understanding and human warmth).
Secondly, knowing the characterological type of the patient, we can more effectively select the strategies of psychotherapeutic and psychocorrectional effects. Third, we can more effectively predict the behavior of patients (for example, understand that the hysteroid is very likely to exaggerate the severity of their symptoms). The examples in this paragraph are deliberately exaggerated in order to show what it is in contrasts. Please do not take it as a guide to action.
For personality research, we use various kinds of projective tests, individual personal questionnaires, and countertransference analysis. I will tell about these methods below.
Research thinking
In this block, we explore, oddly enough, thinking. Or rather, looking for his violations. Or their absence (which can also be diagnostic, for example, by the absence of a slowdown in thought processes, it is possible to exclude the presence of serious endogenous depression).
The main types of disorders can be described as follows: a violation of the operational side of thinking, a violation of the motivational component of thinking, a disorder of the categorical structure of thinking, a decrease in the level of generalization.
The patient may be impaired ability to highlight the main and secondary. And to the question “what’s important in a car”, he will answer “that he is white” or “that I went with my father in a car for fishing”.
Excessive generalizations are possible when the patient is not able to isolate differences at all from different groups of objects, and in perception everything merges into one continuous mess.
Slippage is possible, in which patients, correctly solving a task or reasoning about an object adequately, patients unexpectedly stray from the correct train of thought due to a false association that has arisen, and then are able to continue the reasoning consistently, without correcting the error [12 ].
Reasoning is also a violation of thinking - the tendency of patients to fall into long, unrelated to the subject of reasoning, for example: “I once went to the store, by the way, and you know that the doors in the stores are made of iron, and we mined iron when I served in the army in the Urals, so service in the army is generally a mockery of a person: how can a boy be taken and taken away for two years, etc. ”(the example is fictitious).
There are also motivational-related violations of thinking, which manifest themselves in violation of the hierarchy of needs: if you exaggerate, when a tiger chases a patient, he does not think about how to be saved, but about how Nietzsche's philosophy influenced the development of the Bolshevik party.
There are still violations of the substantive side of thinking - the ideas of relationships (“they are watching me”), nonsense (“I am the illegitimate son of Putin and Merkel, I must own the world”), etc.
To diagnose and assess the degree of disturbed thinking, we use a number of standardized and non-standardized methods for assessing thinking [13], analyzing patient's speech, structured interviews, and clinical conversation.
Memory studies
Everything is simple: there are several types of memory (even not so, there are many ways to classify memory, within each of which there are several types). And almost every one of them we can explore.
In practical work, I share the study of direct memorization (when we ask the subject to memorize something, and then, after a while, to reproduce) and indirect memorization.
In the first case, the standard “de facto” is the method of “Ten words” [14], in which the subject is read ten short unrelated words five times in a row, and after each time he is asked to play them in a random order. Long-term memory is tested by interviewing the subject in an hour.
Indirect memorization is called so because the subject is allowed to use associations to facilitate memorization: for example, to draw pictures that will display an image that allows you to better remember the named word or phrase (for cheaters: you cannot sign).
The trick of the methods of the study of mediated memorization is that, besides, in fact, memory, they very well allow you to explore the mindset (see the previous section) [14]. Below I will show an example.
Intelligence studies
The fact that such intelligence, fierce battles, which are still very far from complete. Personally, I like to use so-called in work. Spearman's G-factor [15] is a value that characterizes the “general intelligence factor”, which is culturally independent and is verified by non-verbal methods. But here the preferences are explained not so much by theoretical views as by the presence of extremely convenient tools - Raven's progressive matrices (which we will discuss below), which can show an adequate assessment of the intellectual abilities of people with different education, cultural background, etc.
As an additional tool, I sometimes use the Wechsler test [16]. The results of this test already depend on the level of education and training of the subject, so by comparing the results of these two tests, we can determine, for example, the degree of pedagogical neglect (when the result is high for Raven and low for Wexler).
Intellect we measure, firstly, to make a diagnosis of mental retardation, secondly, to assess the severity of organic injuries, if any, and, thirdly, to assess intellectual disabilities in schizophrenia. In addition, the strategy of psychotherapeutic or psychocorrectional work with him (some are not able to understand the interpretations given by the psychotherapist) depends on the level of intellect of the subject.
In addition to general intelligence, we also measure social and emotional intelligence. The first is, in simple terms, the ability to correctly understand the behavior of other people. The second is the same, but about emotions.
Indicators on these criteria are important for determining the degree and nature of impaired mental processes, especially in schizophrenia with its emotional-volitional defect.
For the study of social intelligence, I use the test of Guilford, and for emotional - test TAT.
Attention Studies
Attention is the ability of purposeful concentration of perception [17], and it also is impaired. It can independently, besides the will of the test subject, “jump from object to object,” can be depleted, etc.
In general, as a rule, a qualitative assessment of attention can be given simply on the basis of observation of the patient during a clinical conversation and subsequent pathopsychological research. But if I need a quantitative assessment, I use the Schulte tables, the Crepelin score, the Münsberger test, etc.
Attention we appreciate in order to assess the degree of organic disorders, the power of volitional decline in schizophrenia, to identify manic and depressive phases in BAR (as an auxiliary method).
And with these tests it's cool to keep track of the side effects from neuroleptics, trunks and mood stabilizers.
Mental status
Mental status is a characteristic of the patient's current psychoemotional state, i.e. how he feels, what he experiences, how he realizes, where he is, who he is, and why he is there.
We assess our mental status mainly by observation (it is believed that a good specialist can make a diagnosis while the patient passes the post from the door of his office to the chair) and clinical conversation.
Determining mental status, we find out such parameters as accessibility to productive contact (the patient is able to answer questions distinctly and on the topic), orientation in time (what's the date), space (where he is) and self (who is he, why was he ).
Knowledge of mental status allows us to determine the symptom complex, and doctors - to make a diagnosis. Again, with it you can track the dynamics of treatment.
Emotional-volitional sphere
Here we see how the patient is captured by emotions, what kind of emotions are - depression, joy, fear, etc., and also how much he is capable of volitional regulation, i.e. to purposeful continuous activity.
Again, personally, I usually use clinical conversation and observation here, but there are also instrumental assessment methods [18] - such as TAT [18].
But usually the need for instrumental measurements of the parameters of the emotional-volitional sphere does not arise.
We are interested in this area in the sense that information about it helps to identify the correct symptom complex, and repeated research allows us to more accurately track the dynamics of treatment.
So, after we have decided on what and why we are exploring, we can proceed to the most interesting part - the consideration of specific methods of pathopsychological research.
Personal questionnaires. SMIL / RESIN
The SMIL test (standardized multifactor personality research questionnaire) is an adaptation to the domestic realities of the well-known western MMPI test [12]. It includes 566 questions (it takes from one and a half hours to complete), for each of which it is possible to give one of three answers: “yes”, “no”, “I don't know”.
Example of questions from SMIL:
The questions are rather tricky: there are questions to check attentiveness, there are different reformulations of the same statement, there are antagonistic questions. The absolute majority of patients who are first passing SMIL cannot calculate the mechanism of its work, which plays into our hands.
As a result, we get the result in the form of graphs, which are convenient to use to track the effectiveness of treatment. Here is an example of the results of hdablin - the first picture after leaving the mental hospital:
... the second - after about 7-8 months of pharmaco-and psychotherapy in self-treatment mode:
I think it's time to talk about what these charts are, and what they mean. On the abscissa we have the scale. The first three are so-called. confidence scales. The next ten are the main scales.
On the first three scales, we can conclude about how sincere the subject was, whether he tried to put himself in a better or worse light. Sometimes (as in the presented example) it happens that the profile is unreliable formally, but it can be analyzed at the discretion of the interpreter (the gray zone is spelled out in the methodology. But even the patient tried to deceive us (consciously or unconsciously) is usually visible: if he frankly lied, the scale of L (scale of lies) will be increased, if he tried to speak against himself or was anxious - the scale of F (confidence), and if he tried to conform to a certain ideal image, then the scale of K (correction).
The basic information about the subject is given by scales from 1 to 0: Scale of supercontrol, pessimism, emotional lability, impulsivity, masculinity-femininity, rigidity, anxiety, individualism, optimism, introversion [12].
But earlier they were called much clearer: hypochondria, depression, hysteria, psychopathy, masculinity - femininity, paranoia, psychasthenia, schizophrenia, hypomania, social introversion. Agree, so much clearer?
How to interpret this test? Each scale is assigned certain properties. For example, the eighth scale is originality of thinking, the third scale is demonstrativeness, and the second is avoidance behavior.
Up to certain numerical values (65 points), these properties have the appearance of character traits, then - up to 75 - accentuations (this is when, in general, the peculiarity of living does not seem to interfere with living, but in some circumstances is destructive), and even further - this is pathology and perhaps even a mental illness.
Those. on the example of my favorite schizoids, to which I myself belong, 65 points on a scale of 8 - this is originality and singularity, but, here it is 80 on it, - this should be checked for schizophrenia.
According to SMIL, a lot of interesting things can be calculated - to determine the radical of a person, to understand how a person copes with difficulties, what to expect from him in an extreme situation, what kind of work suits him, what motivation prevails - achieving the goal or avoiding failure, etc.
For example, according to the second picture from the illustration above, we can say that the profile smoothed out, somewhat approaching the ideal one (the ideal unattainable profile is a straight line at 50 points), we see that the level of depression has decreased, which has decreased destructive impulsivity, which has decreased very much anxiety, and the characterological basis - a mixed schizo-hysteroid radical - has been preserved.
, , , MMPI HR- . : 2 7 3 4, , « » , , , . , « » , , , .
, . -, . , -. -, : , . -, , .
, ( ), 71 . . , , . .
. .
, , , . , : / . , . . , , .. , .
: , , , . . — , ..
, , - , , , , . : , , , , ..
.
, : , — . , , ( ) , .
«». « ».
: A4 . , ( , ).
, , , , . , . , , .
: a. , b. , c. , d. , e. , f. , g. , h. , i. , j. , k. , l. , m. , n. , o. , p. .
, , ( «») : . .
, hdablin , ( , , , ):
:
: «», («» «», ) , , . « », - . « » « » . , «» .
, [13] , . ? , : (.. ) , , .
. , , :
(). , , .
a) — «, , , »
b) — « , »
c) — «. , — »
d) — « . » ( )
e) — «. , , »
f) — « , »
g) — « »
h) — « » ( )
i) — « , »
j) — « , — »
k) — «» ()
l) — « »
m) — «, » ( )
n) — « »
o) — « »
p) — « » ( ).
, — :
, .
, , , . [13] :
a. , , ( — );
b. ;
c. ( ) ;
d. ;
e. ( )
Other.
, , .
.
. , , , ( ), . « , » , .
, [19]: , , , ..
, , , , , (, , - , , ).
, [19], . : , « — », «» . , , , .
, [19] , , -, , , -, , , ( — , , , , ).
, , , . , . , , ( ) . , , , , , : , , , , ( ).
« ». , , : , , .. Use pre-made fictional characters from works of art, mythology, religion, etc. - prohibited.
, , , : , . , , . , .
, , , — - , , .
, , , hdablin :
, , , , , , , ( , — ). , , .
— :
, , , ( , , ), , .
— ( hdablin ):
, , .
, . . . , , . «», «».
, . . . Those. , .
, , (1). , , (2), .. everything.
. , , , , , .
. .
(3), .
, , .. , . .
, . . . Those. , .
, , (1). , , (2), .. everything.
. , , , , , .
. .
(3), .
, , .. , . .
, , , , , , , , – . , — , ..
- , , . , «».
.
. , , ( ). , , .
( ) [20]:
, , , , , . , . , , -, , , . , , , , . , , , . , , , - , , , . , , , , , , .
:
A healthy person will come up with some plausible plot, without too elaborate details. The schizophrenic is very likely to confine himself to a formal description of the painting in the spirit of "two men cut the third, and the boy faces us."
, , .
.
Quite often it is necessary to test the attention of the patient. The easiest way to do this is by giving it load testing. For example, you can force him to look for numbers in Schulte's tables.
They are cards, which show tables of 5 x 5 cells. Each cell contains a number from 1 to 25 inclusive. Numbers are randomly distributed. The task of the subject is to indicate in turn all the numbers from 1 to 25 in the minimum time. This task is given to the subject five times in a row.
An example of such a table (there are all the necessary numbers, honestly!):
Observing how the subject performs this task, you can collect quite a lot of information about him: the pace of thinking (accelerated, normal, slow), assess the concentration of attention, its stability, exhaustion, type of response, etc. Normally, searching all numbers should take 40-50 seconds.
Tests of intelligence. The Raven Matrices
We need quantitative indicators of intellect for making diagnoses (especially for determining the gradations of mental retardation), for determining the degree of development of a schizophrenic defect, etc.
Personally, I use Raven progressive matrices for this purpose. Their trick is that they measure intelligence precisely as the ability to find solutions, and not as having some kind of knowledge, training in certain areas, etc.
The essence of the test is very simple: you need to select a picture to the sequence. For example, like this:
Again, besides, in fact, the level of intelligence, you can assess a bunch of other factors: attention, fatigue, composure :)
Social intelligence. Guilford test
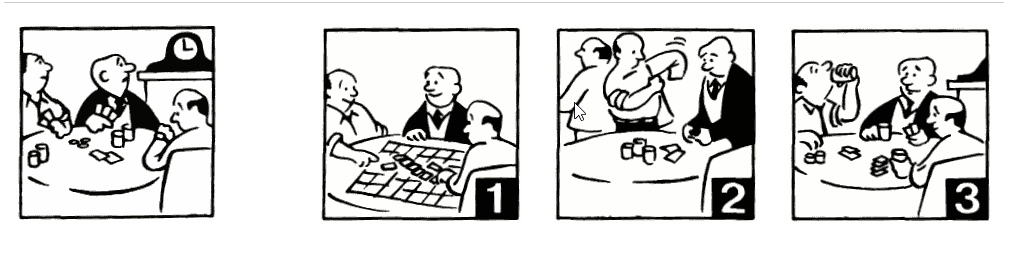
This test shows the ability to understand and predict the behavior of other people. Quite often it happens that the intellect (which is in the previous section) is preserved and even high, and social intelligence is “like a stool” (a characteristic that his psychotherapist gave to hdablin).
The test consists of four categories, in three of which you need to select the appropriate picture. In the first part, you need to choose the end of the story, in the second part - a picture that expresses a certain state or a person’s feeling, in the third one, by the existing phrase, determine who and to whom it could be said and, finally, in the fourth part, select the missing picture to make a related story.
Example of pictures from the first part (here you need to select the following action):
This test quite well shows a person’s ability to recognize and use various social signals and helps in the diagnosis of schizophrenia and mental retardation.
Tests of thinking. Item classification
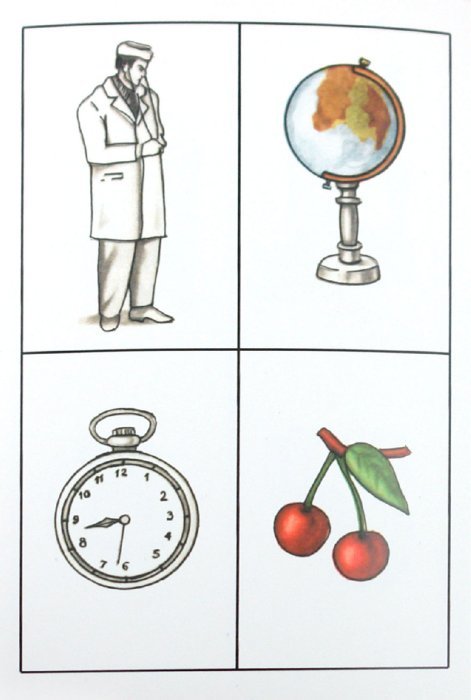
Thinking can be investigated not only through indirect memories and associations, but also directly. A popular technique for this purpose is the “Classification of Objects” test. The subject is offered 71 cards containing images of various objects and the task to group them.
If the subject asks a question about exactly how to group them, they are answered evasively - “as you see fit,” “how do you think is right,” etc.
Cards look like this (in the picture there are four different cards, not one with four items):
A complete list of cards: sailor, baby dress, poppy flower, blacksmith, thermometer, beetle, scissors, swallow, cart, horse, inkwell, watermelon, bicycle, boletus, bow, plane, notebook, doctor, truck, globe, pocket watch, cherry, cup and saucer, sofa, boots, fox, dog, table, goldfish, dog, pan, lamb, bed, centimeter, pigeon, pig, saw, shtangeltsirkul, swan, pine, beetroot, pear, bottle, bookcase, carrot , broom, deciduous tree, cleaning lady, glass, mushroom amanita, cat, books, dipper, fur cap, goat, scales, butterfly, ka RP, goose, apple, wardrobe, child, jacket, elephant, lily of the valley, rooster, bear, skier, motor ship, plum.
Healthy people from these items usually collect the following groups: people, measuring devices, school equipment, kitchen utensils, vehicles, clothing, furniture, vegetables, mushrooms, fruits, flowers, animals, birds, tools, household items.
Patients often create very bizarre associations, for example, a cleaning woman, a wardrobe, a table and a cart are combined on the basis of the presence of something wooden in these images; or table, whatnot, cat, dog and horse - because they have four legs, etc.
Integral approach to patient assessment
So, we have reviewed the main groups of tests that can be used when conducting pathopsychological research. Now it is necessary to tell a little about how their results agree with each other.
The beginning of the examination occurs when the specialist sees the patient (when the latter enters the office). It uses the observation method. An experienced psychologist can make some assumptions about the subject by the first seconds of contact, and he makes them.
Further, anamnesis is collected (aha, again, it is collected twice - by a psychiatrist and a psychologist) and a clinical conversation.
In principle, it may be enough for a good specialist to reasonably expose a certain symptom complex, but instrumental testing is carried out to control and exclude subjective factors.
At this stage, the psychologist already has a certain model of the subject's mind, and is trying to confirm, refute or clarify it. He can conduct a structured interview (it differs from a clinical conversation by having a hard list of questions and a scoring system for evaluating answers to them), after which this model is further refined.
Further, when conducting instrumental testing, there may be evidence in favor of the existing hypothesis regarding the device of the subject's psyche, or its denial. In the latter case, the specialist is required to find an explanation for the discrepancies and include this explanation in the next version of the model.
In general, the essence comes down to the fact that the final positions that will form the basis of the choice of a symptom complex are constantly checked both for logical compatibility between each other and by using different methods.
If, for example, in a SMILER, a test subject has low values on a scale of 3 (emotional lability), and his non-existent animal has a huge peacock tail, eyelashes, and all kinds of curls (a sign of demonstrativeness that should have appeared on a scale 3), then something wrong here.
And then it is necessary either to recognize the unreliable result of SMIL (sometimes the validity scales do not show anything, leaving the decision on the validity or invalid profile at the discretion of the interpreter), or understand that these curls are not curls at all, but some organs, and the tail from possible values (not as a demonstrative, but as a significance of the sexual sphere), or to examine the subject for simulations / dissimulations.
Yes, in pathopsychology there are no such strict and quantitatively definite diagnostic methods, as, for example, in endocrinology, but constant cross-checks allow achieving quite acceptable accuracy.
The boundaries of the norm or what is considered mental health
The World Health Organization identifies the following mental health criteria:
• awareness and sense of continuity, constancy and identity of one’s physical and mental “I”.
• a sense of constancy and identity of experiences in situations of the same type.
• criticality to oneself and one’s own mental production (activity) and its results.
• correspondence of mental reactions (adequacy) to the strength and frequency of environmental influences, social circumstances and situations.
• the ability of self-management behavior in accordance with social norms, rules, laws.
• the ability to plan their own livelihoods and implement these plans.
• the ability to change the way of behavior depending on the change of life situations and circumstances [22].
In principle, I agree with these criteria. But the main thing, in my opinion, is the ability of a person to live without bringing excessive unreasonable difficulties to himself or others. That is why I believe that a happy compensated (that is, a schizophrenic who has found his place in life and firmly established in him) is healthier than a hapless neurotic.
And yes, not always and not all oddities are necessarily a symptom of a mental illness. They can be useful in diagnosis, just as a source of information, but if, for example, you live in central Russia, but all your girls are African, then this is not a reason to consider you sick. Modern psychiatry allows a fairly high degree of variation in behavior.
Is it possible to trick the system
One of the most frequently asked questions to me is whether it is possible to deceive a diagnostician. There is no definite answer to it. It depends, as they say.
If the subject knows the subject (pathopsychology and psychiatry) is much better than a psychologist and a doctor, then, theoretically, yes, he can simulate or dissimulate. It is very difficult: you need to constantly remember about a huge number of factors, one incorrectly set line in the pictograms can completely destroy the image formed by the cheater.
In addition to good knowledge in the subject area, you need to have a very good body control and be a good actor, otherwise it will be seen from nonverbalism that “something is not right here,” and no perfect pictogram will help.
And we sometimes openly provoke our subjects, and they can break under the pressure of emotions, discovering their true nature.
Well, the most difficult thing is pills. In our hospital, the patient cannot but receive medical treatment. He must be given pills, but they don’t say which ones, he doesn’t know which drugs are prescribed for him. And if he wants to deceive someone, he will have to be very hard: you need to understand what these drugs are and how they would affect the person he is portraying.
On the other hand, our hypothetical deceiver is not alone in the department; he may well find a person of the type who depicts, among patients, visually compare the tablets and injections received, and using his observation skills, identify some of the changes that have appeared in the “donor of behavior” since prescription drugs, and copy them. But this is already from the realm of fantasy, for which our psychiatrists could examine me myself :)
Yes, one more thing: one often encounters the fact that someone tries to somehow offend or shock a psychologist, for example, by drawing a genital organ, excrement, and something like that. So, the trick is that, firstly, such an act is itself diagnostic, and, secondly, how this object is drawn can give exactly the same information that could be obtained from an honestly executed drawing .
Self Diagnosis Features
The last question I would like to consider is the possibility of self-diagnosis. Let's do this: it is impossible to diagnose a severe mental disorder in oneself. Just because such disorders significantly distort perceptions of reality, and if you begin to see aliens, then most likely you will have some explanation for this (the literature describes cases of critical attitudes even to the first hallucinations, but this is rare).
For a depressed patient who is on a psychotic level, it seems that he is just objectively bad, and he is genuinely surprised by the stupidity of others who do not understand this, the patient in a manic state sincerely believes that he is such an awesome person, so you can sell an apartment, take a bag loans and arranging a farm for breeding sepules (and it doesn’t matter that no one saw them, they, the others, are simply not good enough for such an activity), an avid PCR specialist can give you a link to clinical studies that “will confirm his need to constantly wash hands, etc.
And the point here is not that a person has no potential knowledge. Even an experienced psychiatrist / medical psychologist cannot self-diagnose himself (in general). Just because the disease creates in our perception "blind spots" that do not allow it to be detected.
However, something a person can do himself. First, he can turn to a specialist as soon as he feels that something is wrong with him. Secondly, to some extent it can withstand light neuroses [21]. Thirdly, he may ask someone to take him to a specialist (for many it is important).
Instead of conclusion
I hope the article fits into the theme of the resource and will find its reader. If you like it, I will try to write the same, but about neuro-and not pathopsychology.
You can ask any questions in the comments, but keep in mind that, firstly, it is impossible to identify a symptom complex (I do not make diagnoses) by commenting, and, secondly, some information from the discharge “but how was it in your mental hospital?” I didn’t I can cite for ethical reasons.
Literature
1. ru.wikipedia.org/wiki/Experimental_psychology
2. Cochrane evidence. Psychological therapies for pathological and problem gambling.
www.cochrane.org/CD008937/DEPRESSN_psychological-therapies-for-pathological-and-problem-gambling
3. Cochrane evidence. Cognitive behavioral therapy for people with asthma. www.cochrane.org/CD011818/AIRWAYS_cognitive-behavioural-therapy-people-asthma
4. Cochrabe evidence. Psychosocial and psychological interventions for postpartum depression.
www.cochrane.org/CD006116/DEPRESSN_psychosocial-and-psychological-interventions-for-postpartum-depression
5. Otte C. Cognitive behavioral therapy in anxiety disorders: current state of the evidence. Dialogues Clin Neurosci. 2011; 13 (4): 413-21.
www.ncbi.nlm.nih.gov/pubmed/22275847
6. Emma Robinson, Nickolai Titov, Gavin Andrews, Karen McIntyre, Genevieve Schwencke, and Karen Solley. Internet Treatment for Generalized Anxiety Disorder: A Randomized Controlled Trial Comparing Clinician vs. Technician Assistance.
www.ncbi.nlm.nih.gov/pmc/articles/PMC2880592
7. Foroushani PS, Schneider J, Assareh N. Meta-review of computerized CBT in treating depression.
www.ncbi.nlm.nih.gov/pubmed/21838902
8. Kudryavtsev, I.A. Comprehensive forensic psychological and psychiatric expertise (scientific and practical guidance). - M .: Publishing House of Moscow. University, 1999, p. 55
9. Medical psychology: Lecture notes / Comp. S.L. Solovyov. - M .: LLC "Publishing AST"; SPb .: Sova LLC, 2004, p. 28
10. N. McWilliams. "Psychoanalytic Diagnostics: Understanding the Personality Structure in the Clinical Process"
11. L.N. Sobchik. “Standardized multifactor method of personality research”
12. Schizophrenic syndrome // Medical psychology: Lecture notes / Compiled by S.L. Solovyov - M-SPb, 2004, p. 44-56
13. B.G. Kherson. “Clinical psychodiagnostics of thinking” - M.:, Meaning, 2014.
14. Rubinstein S. Ya. R 82 Experimental methods of pathopsychology. - M .: ZAO Publishing House EKSMO-Press, 1999. - 448 p. (Series "World of Psychology").
15. Cold MA - "The psychology of intelligence: the paradoxes of research."
16. Wechsler D. Manual for the Wechsler Adult Intelligence Scale. NY, 1955
17. Komarova T. K. Psychology of attention: Textbook.-method. allowance. - Grodno: GrSU, 2002. - 124 p.
18. Blacher V.M., Kruk I.V., Lateral S.N. Clinical Pathopsychology: A Guide for Physicians and Clinical Psychologists. - M .: Publishing House of the Moscow Psychological and Social Institute; Voronezh: Publishing house NPO “MODEK”, 2002.- 512 p. (Series "Library of the psychologist").
19. Wenger A.L. Psychological drawing tests: Illustrated manual. - M .: Vlados-Press, 2003. - 160 p: il.
20. Leontiev D.A. Thematic apperceptive test. 2nd ed., Stereotypical. M .: Meaning, 2000. - 254 s
21. Karen Horney. "Introspection"
22. Eliseev V.V. Psychosomatic diseases. Directory ... - Moscow, 2003.
Source: https://habr.com/ru/post/400869/
All Articles