A cure for medical error, or what tasks the electronic doctor should solve
But it would be good if there was such a program to which he brought his complaints - and immediately found out what and how to be treated ...
So says, probably, every sick geek, faced with some troubles in health care. As well as every medical student who has mastered a computer for 4 years.
But it is impossible. Adults see problems, set tasks and solve them.
In medicine, the problem of medical incompetence, which generates errors that directly translate into our health and quality of life, has been ripening for several decades now. However, this problem is not caused by the general degradation of medicine - on the contrary, there are new ways to diagnose diseases, more effective treatment methods are being developed.
')
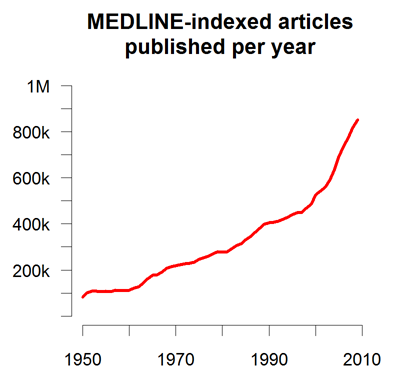
But this is exactly what causes the problem: medical knowledge is becoming more and more, no bright medical head can accommodate them for a long time. Even in their specialty. Let's estimate: every year in the world more than eight hundred thousand medical articles are published in English only. We will remove two thirds of those not directly related to diagnosis and treatment, divide it into a couple of dozen medical specialties, and still there will be several dozens or even hundreds of articles per day for each doctor.
It is not realistic to master, you will say, and you will be right. But what if the inability to get acquainted with all the new information automatically puts doctors - every single one - below the level of modern medicine?
Yes, there is a similar situation in almost all areas of activity - an ordinary Indian from Apvork cannot work at the level of John Carmack, and Aharon’s mechanic from the nearest garage is unlikely to repair the Prius better than a certified Japanese engineer.
Black box
Medicine is a special case. First, because the doctor, in interaction with the patient, acts as a black box: he does not discuss his thoughts and algorithms with the patient, he simply gives a ready-made solution: “follow this recipe.” It is clear that this is due to the complexity and unstructured medical knowledge that does not say anything to the uninitiated. But it is not clear to the aforementioned uninitiated, at what level does a particular doctor work, how well to expect a quality solution from him? Yes, insurance analysts are able to assess the quality of treatment, but only at an “established” level that does not require the use of modern methods. This is an important issue.
Secondly and most importantly, because life is one, and it would be good to take health as seriously as possible. When we eat tons of cookies while sitting at the monitor for hours, it doesn't matter, it is a question of pure subjectivity. But when a doctor may, because of ignorance, miss pseudotuberculosis, mistaking it for the flu, it becomes very important.
The last paragraph may seem soaked with black irony. This is true. But now I looked at myself - red eyes, a belly, a chocolate bar and a drip on the table ... And yes, I am terribly afraid that I once will not recognize cancer at an early stage, at which it can be cured in 90% of cases, and I will die in torment.
You need something that could bring all the knowledge of modern medicine to the doctor.
And to the possible patient! Let not in full, but in some form so that he could apply them, in time to turn to a specialist, or undergo treatment on his own, being in a country with an unfamiliar language or on a long hike. To understand where you can not worry, keeping a good mood and performance, and where you need to urgently run to the doctor (and to which one).
To be sure that the specialist also saw this data, got acquainted with them and correctly interpreted it.
To the doctor was not afraid to make a mistake and did not produce a lot of unnecessary scribbling because of this, did not apply excessive methods of treatment. And the patient knew that going to a doctor would not lead to a deterioration in his health.
Therefore, the main requirement for an electronic doctor is to be useful both to the doctor and to the patient.
We understand that this is in principle possible. Many are already trying to master medical knowledge without having a medical education: the audience of websites dedicated to diseases and their treatment already exceeds the incidence rates recorded by the Ministry of Health: it turns out that almost all registered patients check their doctors, and a significant number of them self-medicate . Surely after all, all these people get some benefit.
Of course, it is impossible to diagnose and treat with high quality using common search engines, since they are not sharpened for this. A search query for diagnostics will include a limited number of complaints that is insufficient for diagnosis, and a request for treatment will lead to general recommendations that do not take into account the characteristics of a particular patient (although some patients guess some common diseases simply by probability theory).
So we got some of the requirements for an e-doctor as a search engine: take a large number of fuzzy data as input, be able to interpret them all.
From search engine to expert system
It is not enough just to find a piece of text, it is necessary to interpret and adapt it for each specific case, that is, for each patient to form a direction for tests, probable diagnoses, the order of visiting doctors and the necessary treatment. Only in this case the time spent on the search will be minimal, and the benefit - the maximum.
But just on this path most of the difficulties are concentrated. If the specialized search engine IBM Watson finds a suitable result in one of many cases, people consider it a victory for technology. But if the same people bring their symptoms into a very powerful Isabel Healthcare ES, which not only searches for diseases, but also assumes diagnoses, they are already outraged that the program does not give out all their diseases, and not in the relevant order as they expect.
I deliberately cited an incorrect example - surely, if Watson is available in extensive testing, the average user will remain dissatisfied. But he illustrates how wide the gap exists in our consciousness between theory and practice, between an imaginary ideal and reality.
However, it may be that any complex tool must be mastered, and the observations of IH users, which I have, relate only to their initial experience. Sooner or later, they, of course, will learn to enter their symptoms, history and results of clinical tests correctly. And then the creator of the electronic doctor will only provide the verifiable accuracy of the results issued by his brainchild.
Developer nightmare
If the data from the user is more or less homogeneous (symptoms, tests are all atomic facts), then the data constituting medical knowledge is extremely difficult to formalize - this is just a fierce nightmare for the developer (At least for those with whom I communicated. Perhaps there are more daring on this resource ... Moderators: the post is not about hiring). In general, see for yourself:
- There are no clear rules for diagnosing diseases. Practically anywhere there is no indication that with such a combination of symptoms such and such a diagnosis is made. Even with options, even with weights of signs, even with conditional operators. Where they exist, this is caused by a decline in the quality of medical education and the need to replace the creative diagnostic search skill with easy-to-learn algorithms. The quality of diagnosis, of course, suffers.
- Moreover, it is extremely rare to indicate Bayesian probabilities of the manifestation of a particular sign in case of a disease. Of the hundreds of medical textbooks, only in one or two I came across constructions of the form “In chronic obstructive bronchitis, persistent cough occurs in 72% of cases, the change in the shape of the nail plates is 65%”. In fact, how to understand when the cough is constant, and when - periodic, but almost constant?
- Many signs may not manifest with the same disease, or manifest in different directions. For example, usually in the inflammatory process there is an increase in the level of leukocytes in the general blood test. But it may not increase. And it may even go down if all the white blood cells left the blood in the tissue to fight the infection, and the body has no new forces (forgive my colleagues for such a vulgar simplification).
- Formal inconsistency of sources of knowledge - it often happens that the approach to diagnosis and treatment varies slightly in different schools. Or, different authors, having the same principles and syndromes in their heads, express them in different ways, the benefit for interpretations is enormous. Why formal - keeping in mind a big baggage of contextual knowledge of physiology, pharmacology, etc., an experienced doctor will not find critical discrepancies in sources. A car based on Tomita Parser will consider them completely different texts.
- Complete confusion in the names. To give just one example of synonyms of the same disease: distireoidnaya ophthalmopathy, malignant exophthalmos, infiltrative ophthalmopathy neurodystrophic exophthalmos, edematous exophthalmos, Graves ophthalmopathy, thyroid ophthalmopathy, thyrotoxic exophthalmos, thyroid exophthalmos, exophthalmic ophthalmopathy, endocrine exophthalmos, euthyroid ophthalmopathy. And in general, it is not so much a disease as a syndrome.
To solve the problem of names, they invented the standard SNOMED CT . But since it turned out to be too large — about 300,000 clinical terms — it became very difficult to use. In other words, standardizing medical terms is a pretty worthless undertaking. In the above example, and so everything is clear (to me). - The rules of credibility of the conclusion on the vast majority of diagnoses are not counted, and therefore, the ideal solution can be taken only by the method of elimination. This gives a very interesting requirement for an e-doctor - to immediately have a base in all sections of medicine, otherwise we will get the Dunning-Kruger effect and negative user experience. Although, if you think about it, what kind of doctor does not suffer from the aforementioned effect, or from the bias of patients?
- In the literature, very little attention is paid to negative signs. If there were many of them, one could take some akinator with a multidimensional array of signs and the problem is solved. But in medicine, a negative sign is essentially equated to an indefinite - “they did not find it,” which means that the tactic of asking questions that reduce entropy as much as possible will lead us into some kind of degenerate field of opportunity, where extreme values are excluded, and the rest can be analyzed only by sequential search.
Hope for a decision
All of the above makes the task of creating an electronic doctor very complicated, which seems to be true - the world does not yet have its high-quality implementation. However, examining most cases of medical error, we see that the use of relatively simple rules available in the machine implementation could exclude it. I will give a couple of examples (excluding or replacing personal data).
A middle-aged woman, the owner of two businesses, has become very tired. She blamed it on the crisis, fired several key employees, sold one of the companies. Three times in the spring she suffered colds of moderate severity. Doctors, one after another, diagnosed neurosis and somatoform depression (that is, considering its physical problems due to the psyche). At some resort, after the procedures associated with pressure drops and intestinal cleansing, the patient became especially ill, and in resuscitation they revealed the destruction of several heart valves. Surgery, disability.
Could she have had rheumatic fever a few months earlier? It is possible, and using a simple algorithm:
- If you complain about tiredness, ask about other mental symptoms: apathy, irritability, restlessness, etc. She would answer that yes, everyone would become annoyed, as many as five good guys fired.
- Why frequent colds? We find out that the temperature lasts almost constantly, and there are often purulent congestion in the glands.
- Have you ever visited doctors before? It always needs to be asked. It turns out there were. To the dentist, already five times. Flux. “But doctor, what does it matter? I appeal to you about general weakness, not teeth. "
It's enough. Chorea. Chronic infection in the teeth and throat. And, if we interpret weakness and temperature as rheumatic heart disease, we get the classic rheumatic triad. It remains to detect the nodules around the joints and the increase in a pair of laboratory parameters, and we win several critical months from the disease: the patient receives an antibiotic and is completely cured.
As we see, correctly asked questions and the simple algorithm connected with them, demanding the minimum participation of the doctor, would render the powerful help.
Another case. A young girl is treated for chronic infections with antibiotics and pyrogenal (now the method is considered obsolete). Pyrogenal, representing the cell wall of dead bacteria, causes a short-term rise in temperature, as if provoking a disease and activation of the body's defense systems. But once having risen to 39-40 degrees, the temperature of the patient has been keeping for five days, without getting lost. What did the doctors do? Assuming that the temperature was caused exclusively by pyrogenal, they were beaten down by more and more powerful means, they pricked the dropper and kept it on home bed rest.
Fortunately, it did well here: the patient's husband took advantage of one of the imperfect online diagnostics, with a simple algorithm “if there is a high fever, you need to ask about the rash”. A rash was found - symmetrical, punctate, tied with the time of year and stay in the village, then went straight to the infectious diseases hospital.
Any doctor will find many similar cases in his practice, and this gives hope that an electronic doctor is quite possible. That one day people will stop doing self-medication in Google and listen to the advice of familiar attendants.
Source: https://habr.com/ru/post/398147/
All Articles