Astigmatism - methods of correction
You live, do not be sad, look at the world with narrowed eyes, and suddenly you are told that you have astigmatism. Astigmatism - optics of the eye with irregular focusing, when there is no clarity on the retina due to distortions in the cornea or lens of the eye. It is impossible to make such a diagnosis on your own - an ophthalmologist discovers it. And the question arises - what to do with it? Wear glasses or contact lenses, train from morning to night as the Internet recommends or give yourself in the hands of surgeons to “correct” the sight?
And another option is to do nothing, continue to live as before, nothing hurts.

An important rule is to understand which part of the eye this optical problem is associated with. The method of correction or treatment of astigmatism will depend on this.
The second important rule is to understand how it changes over time, since astigmatism may be one of the symptoms of eye disease that require treatment.
')
The third important rule is at what age is it detected and what is its magnitude. In children, it requires constant correction with glasses from a very early age and, often, additional classes on the apparatus. If this is not done, then the eye will become "lazy"; amblyopia will appear - a decrease in vision, which cannot be corrected by any means of correction at an older age.
Surgical treatment - the lot of an adult over 18 years of age. If the cornea is healthy and just a “curve” - welcome to laser vision correction. If the cornea is thin and sore, we heal, strengthen and correct with other methods.
If astigmatism causes blurred vision, the eyes get tired quickly, the contours of objects blur or split, there is dryness and pain in the eyes with minor visual loads, the vision deteriorates at dusk - you need astigmatic glasses.
Astigmatic glasses are also called cylindrical, this is the simplest, relatively economical and effective method of correction.
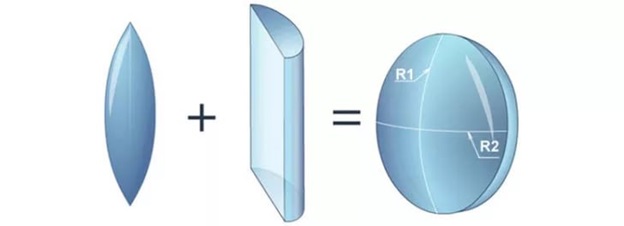
Such a selection is a multi-stage process of examination of the optical system of the eye. The specificity of astigmatic lenses is that they must correct vision immediately and vertically and horizontally with different optical power of the lenses. Therefore, astigmatic lenses have an uneven bend, resembling an oval or a stretched sphere.
At the beginning, the optics of the eye should be examined on several instruments, including an autorefractometer, aberrometer, keratometer, corneal topograph, slit microscope
I wrote about how this happens here (because the diagnostics for glasses and laser is the same): “We got to the side effects of laser vision correction - and before the diagnosis”
Having received a primary idea of the degree, type and type of astigmatism, the oculist checks visual acuity without correction and with maximum correction with each eye separately, then with two eyes. Choose the option of glass that provides the best clarity of vision. Then necessarily follow the stage of adaptation to the selected lenses.
If the selection of astigmatics is carried out for the first time, especially in adults or elderly people, then it is very important to take into account the maximum tolerable value of astigmatic lenses. Otherwise, when wearing, dizziness, visual discomfort, inability to move in space will occur. Often, in these cases, temporary intermediate glasses with incomplete correction are prescribed to patients, and then they gradually increase after the end of the adaptation period.
With high degrees of myopia and farsightedness, combined with astigmatism, it is more difficult to pick up glasses, the period of getting used to them may be delayed. This ophthalmologist must warn you in advance.
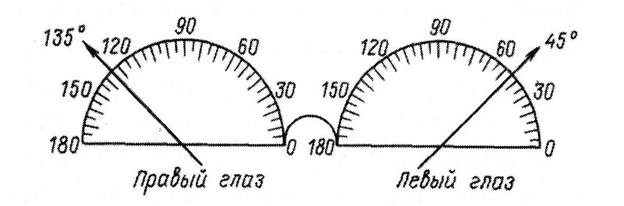
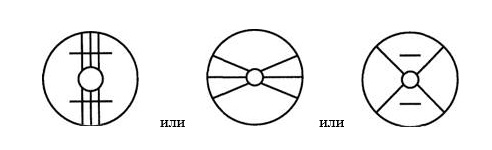
Scheme to indicate the position of the axes of the corrective glasses with astigmatism
Well, these glasses are not without flaws - as well as common with all points (changing a person’s appearance, misting of lenses, the need for periodic replacement, limiting the field of view, etc.), as well as specific flaws.
Astigmatic glasses are difficult to select, the cost of cylindrical lenses is high, time is needed for adaptation and, in some cases, their complete intolerance.
From an aesthetic point of view, the lenses do not affect the appearance and do not limit the view, so they have many active users. In addition, there are still a couple of obvious advantages from a medical point of view:
What is wrong with the lenses is their daily presence on the surface of the cornea.
I wrote about all the problems that contact lens users may encounter in the last post: What is more dangerous: wearing contact lenses or laser correction?
Much in this case depends on your thoroughness, cleanliness and wealth. Daily contact lenses are better than reusable ones, but they are more expensive. But in the long run, there is every chance of earning an infectious, traumatic, or dystrophic eye condition.
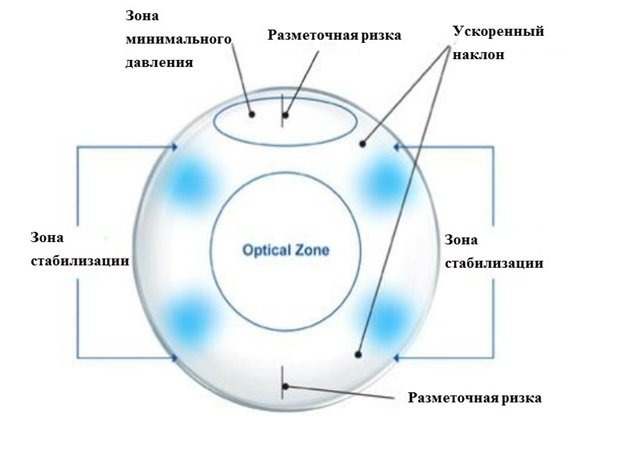
When choosing a type of contact lenses with astigmatism, ophthalmologists often advise soft toric ones. Correction of a strong meridian with such lenses is combined with correction of myopia or hyperopia. The special geometry of the lenses keeps the product in a stable position, making it independent of eye movements. Therefore, it affects only the desired meridian.
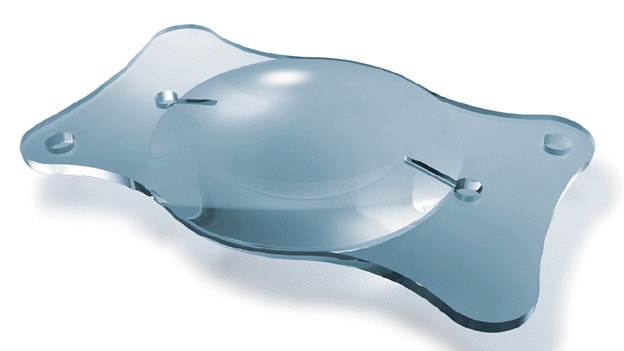
Astigmatic lens configuration
With the ineffectiveness of attempts at a conservative correction recommended surgery using a laser.
Laser vision correction for astigmatism is a great way to get rid of glasses or contact lenses for medical reasons. I draw the attention of my patients to the fact that astigmatism does not make it possible to see clearly either at close or far distances, and this is another reason to part with this problem forever.

What way to carry out the correction should be solved depending on the anatomy and physiology of the eye after a comprehensive diagnostic examination.
Correction by all currently existing methods is possible: ReLex SMILE, FLEX, FemtoLASIK, LASIK or PRK. The features of these types of correction are described in detail in a series of previous posts:
→ Laser that cuts inside the cornea: ReLE procedure at the physical level
→ Telemetry from a laser for vision correction: a complete operation with comments (not for the faint of heart)
→ History of vision correction operations: comparison of risks and side effects
→ A couple more unobvious things that you might not be told before laser vision correction
→ FAQ about laser correction ReLEx SMILE: yes, in Russia there is, but no, in Russia there isn’t
→ We got to the side effects of laser vision correction - and even before the diagnosis
→ Operating equipment for vision correction
What you need to pay attention to - the “sick” cornea is a contraindication to any type of laser surgery, including the most modern and gentle ReLex SMILE. And astigmatism is one of the symptoms of a “diseased” cornea in an explicit or hidden state (keratoconus). Therefore, sighting diagnostics is important in any case. If the cornea does not allow for laser vision correction, then in this case the issue can be resolved by implanting phakic lenses.
When myopia or hyperopia is attached to astigmatism, there is another surgical method as an alternative option - to put an intraocular contact lens on your own lens, which is not visible externally and does not need to be removed. This option is suitable for those cases where the thickness of the cornea is either not enough, or you cannot interfere with its structure. Thus, one simple procedure can solve the problem of both high myopia and astigmatism.
These implants are created from biocompatible materials that can live inside the eye for decades until the space is enough or there is no cataract. Such lenses are “grown” individually with given parameters, for example, “minus” and with the necessary astigmatic component and implanted into the eye in a certain position.
The optical diameter of the lens is from 5.5 mm to 4.65 mm, depending on the size of the myopia - the larger the minus, the smaller the optical zone, so as not to “thicken” the lens too much.
The length of the supporting (haptic) part can be 115 mm, 120 mm, 125 mm, 130 mm - this is calculated individually, based on measurements of external landmarks and internal spaces. Astigmatism correction is possible from 1 to 6 diopters and at the same time very high quality of vision is achieved.
The details of the augmentation of phakic lenses are described in a post earlier:
→ “Augmentation” eyes: what do we build into it today, and what else will remain under it
→ Calculation of intraocular phakic lenses (embedded in the eye) - we continue about the eye and its biomechanics
By the way, implantation (as well as the calculation) of this kind of lenses requires skill and skill. In my life I had to extract someone else's phakic lenses, set “backwards” or “upside down”.
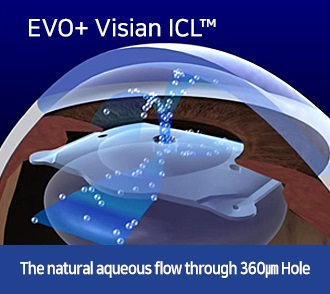
In modern models of phakic lenses there is a hole in the center for the free movement of intraocular fluid:
In the 1980s Academician Svyatoslav Fedorov and co-authors developed a mathematical model of corneal deformity after performing metered keratotomy incisions on the front of the cornea. According to this model, the operation — anterior radial keratotomy — ie, vision correction by notches on the cornea.
The principles of anterior dosed keratotomy were used to correct various forms of astigmatism. For the correction of simple myopic astigmatism, the so-called tangential keratotomy was developed - reducing the refraction in the cross section perpendicular to the incision direction, and radial-tangential keratotomy was used to correct complex myopic astigmatism.
It looked schematically like this - like sliced pie:
This was done manually by splintering the blades to a dosed depth - hence the results were rather approximate.
Today, with the advent of femtosecond technologies (ultrashort laser pulses) without heating and damaging the surrounding tissues with a number of expanding cavitation bubbles, we can produce a tissue incision (femtodissection) as a universal scalpel. With the help of a femtosecond laser, we increase the clinical accuracy, safety, and effectiveness of this method in correcting corneal astigmatism, as compared to “traditional” keratotomy.
Today, we can use this alternative method in clinical situations in which it is almost impossible to perform the required spectacle or contact correction due to pronounced irregularity of the cornea, as well as to extract lenticules or excimer laser refractive surgery due to insufficient corneal stroma thickness for correcting myopic astigmatism. This method is the most "budget" version of the correction.
Everything I wrote about above concerned only changing the shape of some part of the eye or adding something to it. But there is a way to correct the optics of the eye by removing something and replacing it with an implant with additional useful properties.
So, removing your own lens and replacing it with an artificial astigmatic. They are also called cylindrical or toric.
How does the operation to remove the lens occur and in what cases I need to write it here:
→ Cataract: it is waiting for you personally (if you live, of course)
→ Implant an artificial lens (you will need it after 60 years)
By the way, if a patient has lens astigmatism, then he will disappear after the removal of his own lens.
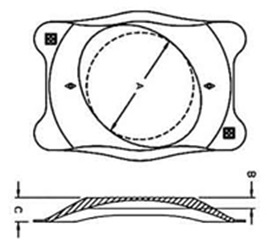
But if the cornea is uneven, then an artificial lens-lens, the optical part of which has a cylindrical additive like a lens for glasses with astigmatism - a toric intraocular lens (IOL) can help.
It looks like this:
Are there any other options:

The point is that toric IOLs, in addition to biconvex spherical optics, have a toric component on the back surface, and a strong axis is marked with two coaxial marks for positioning the lens at the end of the operation.
Thus, we get a one-step correction of aphakia and corneal astigmatism using toric IOLs, the use of which allows us to avoid additional corneal refractive operations with residual astigmatism.
The main requirements for such lenses are not only the neutralization of corneal astigmatism immediately after surgery, but also the need for a stable position of the IOL in the capsular bag for a long time. The rotational instability of toric IOL models causes a significant decrease in vision in the postoperative period. The most common cause of rotational instability of an IOL is the wrinkling of the capsular bag due to the development of a fibrous process, as a result of which the lenses “turn” around its axis in a clockwise direction.
In advanced operating microscopes, the image of the desired axis for the orientation of the lens is projected onto the image in the microscope. Like this:
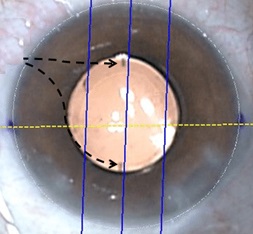
The image in the microscope with the projection of labels in the desired meridian
Operations such as crosslinking and implantation of intracorneal segments also affect the optics of the eye. They lead to the strengthening of the corneal framework, to the modeling of a more regular and regular cornea, reducing its curvature.
In which cases it is necessary to look here: Keratoectasia (keratoconus, "convex cornea"): what is it and what to do with it
To calculate the required length, thickness and geometry of the segments, there are nomograms and various formulas to help the surgeon, but the accuracy of such calculations is not as high as with laser correction or lens implantation. The main goal in this case is medical, and the improvement of optics is a bonus to it.
The result will be just a few conclusions:
And another option is to do nothing, continue to live as before, nothing hurts.
An important rule is to understand which part of the eye this optical problem is associated with. The method of correction or treatment of astigmatism will depend on this.
The second important rule is to understand how it changes over time, since astigmatism may be one of the symptoms of eye disease that require treatment.
')
The third important rule is at what age is it detected and what is its magnitude. In children, it requires constant correction with glasses from a very early age and, often, additional classes on the apparatus. If this is not done, then the eye will become "lazy"; amblyopia will appear - a decrease in vision, which cannot be corrected by any means of correction at an older age.
Surgical treatment - the lot of an adult over 18 years of age. If the cornea is healthy and just a “curve” - welcome to laser vision correction. If the cornea is thin and sore, we heal, strengthen and correct with other methods.
How to choose glasses for astigmatism
If astigmatism causes blurred vision, the eyes get tired quickly, the contours of objects blur or split, there is dryness and pain in the eyes with minor visual loads, the vision deteriorates at dusk - you need astigmatic glasses.
Astigmatic glasses are also called cylindrical, this is the simplest, relatively economical and effective method of correction.
Such a selection is a multi-stage process of examination of the optical system of the eye. The specificity of astigmatic lenses is that they must correct vision immediately and vertically and horizontally with different optical power of the lenses. Therefore, astigmatic lenses have an uneven bend, resembling an oval or a stretched sphere.
At the beginning, the optics of the eye should be examined on several instruments, including an autorefractometer, aberrometer, keratometer, corneal topograph, slit microscope
I wrote about how this happens here (because the diagnostics for glasses and laser is the same): “We got to the side effects of laser vision correction - and before the diagnosis”
Having received a primary idea of the degree, type and type of astigmatism, the oculist checks visual acuity without correction and with maximum correction with each eye separately, then with two eyes. Choose the option of glass that provides the best clarity of vision. Then necessarily follow the stage of adaptation to the selected lenses.
If the selection of astigmatics is carried out for the first time, especially in adults or elderly people, then it is very important to take into account the maximum tolerable value of astigmatic lenses. Otherwise, when wearing, dizziness, visual discomfort, inability to move in space will occur. Often, in these cases, temporary intermediate glasses with incomplete correction are prescribed to patients, and then they gradually increase after the end of the adaptation period.
With high degrees of myopia and farsightedness, combined with astigmatism, it is more difficult to pick up glasses, the period of getting used to them may be delayed. This ophthalmologist must warn you in advance.
Scheme to indicate the position of the axes of the corrective glasses with astigmatism
Well, these glasses are not without flaws - as well as common with all points (changing a person’s appearance, misting of lenses, the need for periodic replacement, limiting the field of view, etc.), as well as specific flaws.
Astigmatic glasses are difficult to select, the cost of cylindrical lenses is high, time is needed for adaptation and, in some cases, their complete intolerance.
What is better with astigmatism - glasses or lenses?
From an aesthetic point of view, the lenses do not affect the appearance and do not limit the view, so they have many active users. In addition, there are still a couple of obvious advantages from a medical point of view:
- First, their strength can be changed if myopia progresses.
- Secondly, in a contact lens, visual acuity is often higher, since the lenses are placed directly on the cornea, and there is a distance between the spectacle lenses and the cornea.
- Thirdly, correction by lenses is possible with a big difference in the optics of two eyes, because the image size on the retina will be the same.
- And finally, with moderate astigmatism up to 1.5 diopters, it is easy to achieve correction with conventional spherical lenses by leveling the surface with a tear.
What is wrong with the lenses is their daily presence on the surface of the cornea.
I wrote about all the problems that contact lens users may encounter in the last post: What is more dangerous: wearing contact lenses or laser correction?
Much in this case depends on your thoroughness, cleanliness and wealth. Daily contact lenses are better than reusable ones, but they are more expensive. But in the long run, there is every chance of earning an infectious, traumatic, or dystrophic eye condition.
When choosing a type of contact lenses with astigmatism, ophthalmologists often advise soft toric ones. Correction of a strong meridian with such lenses is combined with correction of myopia or hyperopia. The special geometry of the lenses keeps the product in a stable position, making it independent of eye movements. Therefore, it affects only the desired meridian.
Astigmatic lens configuration
With the ineffectiveness of attempts at a conservative correction recommended surgery using a laser.
Laser vision correction for astigmatism
Laser vision correction for astigmatism is a great way to get rid of glasses or contact lenses for medical reasons. I draw the attention of my patients to the fact that astigmatism does not make it possible to see clearly either at close or far distances, and this is another reason to part with this problem forever.
What way to carry out the correction should be solved depending on the anatomy and physiology of the eye after a comprehensive diagnostic examination.
Correction by all currently existing methods is possible: ReLex SMILE, FLEX, FemtoLASIK, LASIK or PRK. The features of these types of correction are described in detail in a series of previous posts:
→ Laser that cuts inside the cornea: ReLE procedure at the physical level
→ Telemetry from a laser for vision correction: a complete operation with comments (not for the faint of heart)
→ History of vision correction operations: comparison of risks and side effects
→ A couple more unobvious things that you might not be told before laser vision correction
→ FAQ about laser correction ReLEx SMILE: yes, in Russia there is, but no, in Russia there isn’t
→ We got to the side effects of laser vision correction - and even before the diagnosis
→ Operating equipment for vision correction
What you need to pay attention to - the “sick” cornea is a contraindication to any type of laser surgery, including the most modern and gentle ReLex SMILE. And astigmatism is one of the symptoms of a “diseased” cornea in an explicit or hidden state (keratoconus). Therefore, sighting diagnostics is important in any case. If the cornea does not allow for laser vision correction, then in this case the issue can be resolved by implanting phakic lenses.
Intraocular Contact Lens for Astigmatism Correction
When myopia or hyperopia is attached to astigmatism, there is another surgical method as an alternative option - to put an intraocular contact lens on your own lens, which is not visible externally and does not need to be removed. This option is suitable for those cases where the thickness of the cornea is either not enough, or you cannot interfere with its structure. Thus, one simple procedure can solve the problem of both high myopia and astigmatism.
These implants are created from biocompatible materials that can live inside the eye for decades until the space is enough or there is no cataract. Such lenses are “grown” individually with given parameters, for example, “minus” and with the necessary astigmatic component and implanted into the eye in a certain position.
The optical diameter of the lens is from 5.5 mm to 4.65 mm, depending on the size of the myopia - the larger the minus, the smaller the optical zone, so as not to “thicken” the lens too much.
The length of the supporting (haptic) part can be 115 mm, 120 mm, 125 mm, 130 mm - this is calculated individually, based on measurements of external landmarks and internal spaces. Astigmatism correction is possible from 1 to 6 diopters and at the same time very high quality of vision is achieved.
The details of the augmentation of phakic lenses are described in a post earlier:
→ “Augmentation” eyes: what do we build into it today, and what else will remain under it
→ Calculation of intraocular phakic lenses (embedded in the eye) - we continue about the eye and its biomechanics
By the way, implantation (as well as the calculation) of this kind of lenses requires skill and skill. In my life I had to extract someone else's phakic lenses, set “backwards” or “upside down”.
In modern models of phakic lenses there is a hole in the center for the free movement of intraocular fluid:
Tangential keratotomy - correction in the "simplified" version
In the 1980s Academician Svyatoslav Fedorov and co-authors developed a mathematical model of corneal deformity after performing metered keratotomy incisions on the front of the cornea. According to this model, the operation — anterior radial keratotomy — ie, vision correction by notches on the cornea.
The principles of anterior dosed keratotomy were used to correct various forms of astigmatism. For the correction of simple myopic astigmatism, the so-called tangential keratotomy was developed - reducing the refraction in the cross section perpendicular to the incision direction, and radial-tangential keratotomy was used to correct complex myopic astigmatism.
It looked schematically like this - like sliced pie:
This was done manually by splintering the blades to a dosed depth - hence the results were rather approximate.
Today, with the advent of femtosecond technologies (ultrashort laser pulses) without heating and damaging the surrounding tissues with a number of expanding cavitation bubbles, we can produce a tissue incision (femtodissection) as a universal scalpel. With the help of a femtosecond laser, we increase the clinical accuracy, safety, and effectiveness of this method in correcting corneal astigmatism, as compared to “traditional” keratotomy.
Today, we can use this alternative method in clinical situations in which it is almost impossible to perform the required spectacle or contact correction due to pronounced irregularity of the cornea, as well as to extract lenticules or excimer laser refractive surgery due to insufficient corneal stroma thickness for correcting myopic astigmatism. This method is the most "budget" version of the correction.
Astigmatic lenses - implants with cylindrical optics
Everything I wrote about above concerned only changing the shape of some part of the eye or adding something to it. But there is a way to correct the optics of the eye by removing something and replacing it with an implant with additional useful properties.
So, removing your own lens and replacing it with an artificial astigmatic. They are also called cylindrical or toric.
How does the operation to remove the lens occur and in what cases I need to write it here:
→ Cataract: it is waiting for you personally (if you live, of course)
→ Implant an artificial lens (you will need it after 60 years)
By the way, if a patient has lens astigmatism, then he will disappear after the removal of his own lens.
But if the cornea is uneven, then an artificial lens-lens, the optical part of which has a cylindrical additive like a lens for glasses with astigmatism - a toric intraocular lens (IOL) can help.
It looks like this:
Are there any other options:
The point is that toric IOLs, in addition to biconvex spherical optics, have a toric component on the back surface, and a strong axis is marked with two coaxial marks for positioning the lens at the end of the operation.
Thus, we get a one-step correction of aphakia and corneal astigmatism using toric IOLs, the use of which allows us to avoid additional corneal refractive operations with residual astigmatism.
The main requirements for such lenses are not only the neutralization of corneal astigmatism immediately after surgery, but also the need for a stable position of the IOL in the capsular bag for a long time. The rotational instability of toric IOL models causes a significant decrease in vision in the postoperative period. The most common cause of rotational instability of an IOL is the wrinkling of the capsular bag due to the development of a fibrous process, as a result of which the lenses “turn” around its axis in a clockwise direction.
In advanced operating microscopes, the image of the desired axis for the orientation of the lens is projected onto the image in the microscope. Like this:
The image in the microscope with the projection of labels in the desired meridian
Crosslinking and Corneal Rings - Effects on Astigmatism
Operations such as crosslinking and implantation of intracorneal segments also affect the optics of the eye. They lead to the strengthening of the corneal framework, to the modeling of a more regular and regular cornea, reducing its curvature.
In which cases it is necessary to look here: Keratoectasia (keratoconus, "convex cornea"): what is it and what to do with it
To calculate the required length, thickness and geometry of the segments, there are nomograms and various formulas to help the surgeon, but the accuracy of such calculations is not as high as with laser correction or lens implantation. The main goal in this case is medical, and the improvement of optics is a bonus to it.
The result will be just a few conclusions:
- The sooner the correction of astigmatism is made, the less likely the development of complications, including a sharp deterioration in vision, the development of a "lazy" eye, the formation of strabismus.
- Astigmatism correction methods are many and the choice is always individual.
- For the correct selection it is necessary to expend some time and effort.
- Early correction of glasses is the key to eye health. It is necessary to regularly visit an ophthalmologist to monitor the state of vision.
Source: https://habr.com/ru/post/374011/
All Articles