Part 4.1 We return the sight. From points to the excimer laser

I apologize to all those who have been waiting for this article for a long time. Preparation of materials requires a lot of time and labor. In this article I will try to talk about all methods of vision correction that exist at the moment. We will go from the first points of the XIII century to modern laser correction methods such as femto-LASIK and PRK.
If you have not read the previous articles of the cycle, then I would recommend to familiarize yourself with the second part first. It is precisely in it that the main visual impairment and the biological basis of our vision are analyzed. The volume of the article was very large, so I decided to split it into two parts to facilitate the perception.
All who are interested - welcome under cat.
Other parts
Part 1. Unboxing VisuMax - femto laser for vision correction
Part 2. How many megabits / s can be passed through the optic nerve and what is the resolution of the retina? Some theory
Part 3. Meet - laser called Amaris. Moving and first awakening of VisuMax
Part 4.2 We return the sight. From points to the excimer laser
Table of contents:
')
Problem and solution methods
Simple solutions. Add a lens
We answer questions
In the next part:
We change the cornea
- Features of the method
- Orthokeratology
- Keratotomy
- Lasik
- femto-LASIK
- PRK
- trans-PRK
- ReLEx SMILE
- ReLEx Flex
When the cornea is missing
- Features of the method
- Phakic lens implantation
- Implantation of an artificial lens - IOL
Refraction OK
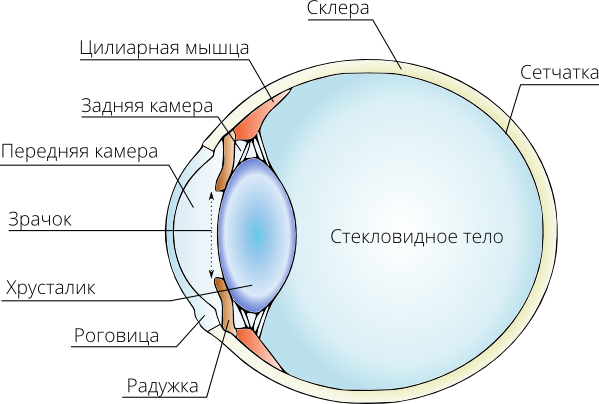
The eye is a complex optical system. The main elements that are directly involved in focusing the image on the retina:
- Cornea
- Front camera
- Pupil as a diaphragm
- Rear camera
- Lens
- Vitreous humor
On the one hand, every change in any area will inevitably degrade the quality of the image on the retina. On the other hand, such a close relationship makes it possible to correct vision by acting on other elements that are not the cause of the disturbance. For example, when myopia eyes grows along its optical axis. Putting on the glasses, we adjust the image by focusing it on the retina, but the shape of the eyeball is still stretched.
Points of impact on the problem

We can identify several areas where you can correct refraction with minimal cost:
- Add corrective lense glasses
- Add corrective contact lens
- Change the curvature of the cornea
- Implant a phakic lens into the anterior or posterior chamber of the eye
- Replace the lens with an artificial one with another optical power
Points in the Middle Ages

The history of points began a long time ago. Optical properties of crystals of rock crystal and other minerals since ancient times were used to increase objects. Optical lenses from rock crystal archeologists found at the excavations of Troy, Crete, in the Syrian desert, under the Mesopotamian hills. Ancient Greek philosophers wrote about the use of "crystals for the eyes". The Roman historian Pliny the Elder, who died during the eruption of Vesuvius, said that "the emperor Nero watched gladiatorial battles through smaragd", i.e. emerald lens.
However, all these artificial lenses were not medical in nature and did not serve for the correction of vision. The exact place of the invention of the glasses is not exactly known. Most researchers agree that this discovery took place simultaneously in several countries of central Europe. Despite this, a lot of historical evidence points to Italy of the XIII century. Glassmakers of that era were famous for their glass work. It is likely that it is thanks to them that this attribute has spread to the rest of the world.
There is evidence that the idea of creating glasses belongs to a Florentine monk and dates back to 1280. Near one of the Florentine churches is his grave with the inscription: "Here lies Salvino Armati, the inventor of glasses."
Glasses at that time were extremely expensive, but the ordinary commoner simply had nothing to read. Most of them were illiterate, and the mass book printing was still waiting for Guttenberg.
Modern glasses

Now glasses use all the achievements of modern technology. These are rims of titanium alloys with shape memory, and light polymers as eyeglass lenses, which, thanks to a high refractive index, make the glasses very thin. In principle, it is glasses that can be considered as a method for correcting refractive disorders, which makes it possible to achieve a good quality of vision without affecting the organ of vision itself.
I can not fail to mention the popular myth that glasses can accelerate the development of myopia and their wearing should be avoided as much as possible. As we already know, the cause of myopia in most cases is an increase in the linear size of the eyeball. Adding points only allows you to properly focus the light flux. Wearing an eye does not affect their shape. Moreover, the refusal to wear glasses with severe myopia leads to constant overload of the ciliary muscle of the lens, which painfully tries to “adjust the image normally,” but cannot because of the gross discrepancy between the focal length of the eye and its capabilities. All this can lead to aggravation of the problem with accommodation spasm.
Very often I hear the concept: “I went without glasses and saw something. I wore glasses, looked like six months, now I can’t do without them, although before that everything was tolerable. ” Blurred vision is a delusion. The human brain is a very flexible tool. Of the two series of frames of “video” of disgusting quality, he manages to extract bits of useful information. All myopic acquaintances are familiar with recognizing those who are familiar from their silhouettes, movement patterns, etc. When a person wears glasses for a long time, the brain discards unnecessary "modules" to save resources. That is why it is so difficult for a person to break points off afterwards. Here, rather, the question arises whether it should be done at all.
You can have different attitudes to expensive and cheap frames, but I definitely urge you not to save on high-quality lenses for them. As well as optics for good lenses, lenses of good manufacturers cannot be very cheap. Especially if correction with astigmatism compensation is required. A nice bonus is the presence of additional coatings that reduce chromatic aberrations, which increase strength, etc.
When choosing a lens, you need to remember that the thickness of the lens, other things being equal, depends on the refractive index of its material. That is, by choosing high-index lenses, you can get a full-fledged correction with a much smaller thickness. True, this will have to come to terms with the enhancement of chromatic aberrations, although the manufacturer is trying to deal with it. The reason for such aberrations is the difference in the refraction of light of different wavelengths.
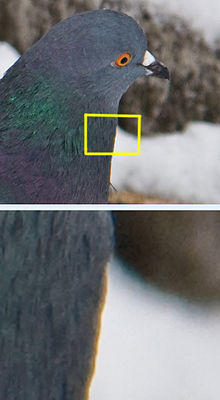
An example of chromatic aberration.
It would be useful to use single or double aspherical optics. Such lenses can significantly reduce geometric distortion at the edges of the lens. Of course, this will also increase the final price. For myself, I stopped at the lenses of the Japanese company Hoya. They cost me 2 times cheaper than those of Zeiss, not inferior in quality.
Contact lenses

Contact lenses as a class appeared a long time ago. Leonardo da Vinci expressed his thoughts about them, and the first incarnation of blown glass was created by the German glassblower Augustus Muller in 1887. A year later in 1888, Adolf Fick, an ophthalmologist, applied this invention in practice. First on rabbits, then on himself and then on volunteers. The materials have changed and improved, but in the process it turned out an unpleasant feature of contact lenses - they worsen the cornea gas exchange.
The cornea is a transparent tissue and cannot afford to be overgrown with food vessels. Therefore, the exchange of metabolic products and oxygen for breathing, it carries out by washing the tear fluid and the circulation of fluid in the anterior chamber. Contact lenses do not contribute to this process in any way, no matter how the manufacturers practice “80% airborne” slogans, “first * breathing ** contact lenses” and so on. Experience suggests that patients who choose contact correction, as a method for solving the problem of myopia, inevitably come to problems with the cornea - keratitis, dry eye syndrome, increase the chances of contact infection and a number of other problems. For example, a pause in wearing lenses for at least 2 weeks is required before laser correction. And this in the absence of other health problems of the cornea.

Contact lenses are divided into hard and soft . Rigid lenses are distinguished by their form stability and make it possible to effectively solve the problems of correcting complex astigmatism and a number of other problems. However, due to poor gas permeability, they are used quite rarely. Soft lenses are divided into two main groups depending on the material: hydrogel and silicone-hydrogel.
Hydrogel lenses are divided into groups, depending on the water content:
- low water lenses (<50%)
- medium water lenses (about 50%)
- high water lenses (> 50%)
The higher the concentration of water in a hydrogel lens, the better it passes oxygen, however, after 70% the lens becomes inconvenient in operation due to the extreme instability of the form.
Silicone-hydrogel lenses have more optimal characteristics and do not have a relationship between water content and gas permeability.
The ability of a contact lens to pass oxygen is characterized by a special coefficient Dk / t (Dk is the oxygen permeability of the lens material, and t is the thickness of the lens in the center). For hydrogel lenses Dk / t usually lies in the range of 20-30 units. This is enough for daytime wear. In order for the lenses to be left on the eyes at night, much larger values are required. Silicone hydrogel contact lenses have Dk / t on the order of 70-170 units. In general, night wear is a huge problem. With the century closed, the oxygen concentration drops significantly. If we add a contact lens to this, the cornea will suffer from oxygen starvation. Therefore, if you are not alone in a dark forest surrounded by hedgehogs and Christmas trees, and the bag with solutions has not been dragged off by raccoons, then it is highly desirable not to use lenses at night. Handbook of gas permeability of various lenses (thanks to f1ac )
A very important problem is the correction of astigmatism. If a person’s cornea has a regular, symmetrical shape, then he has no problems with conventional contact lenses. The orientation of such a lens relative to the axis of symmetry is not important. However, sometimes besides myopia there is asymmetry of the cornea or lens, which results in astigmatism. In such patients, the orientation of the lens is very important. The main task is to compensate for the natural asymmetry along the respective axes. Previously, such patients were prescribed extremely rigid contact lenses due to the stability of their shape and ease of orientation. Unfortunately, the transmission of oxygen in such lenses is minimal. Modern materials have allowed to create soft toric lenses , which themselves take the necessary position on the cornea, rotating under the action of gravity.
There are various methods of stabilizing the lens:
- Periballast - the lens has thinning zones along the upper and lower edges, located under the eyelids, which hold the lens in the desired position.
- prismatic ballast - a thickening in the lower part of the lens, which under the action of gravitational forces causes the lens to be in the desired position. But when the body changes its position from vertical to horizontal and vice versa, the lens also shifts under the action of gravity.
- clipping or truncation — a segment is clipped at the bottom of the lens. The resulting slice lens is located on the edge of the lower eyelid.
Here, too, is not without problems. If the lens of glasses can easily maintain its orientation relative to the eye due to the rigidity of the structure, then the contact lens under the action of gravity can rotate when the head is tilted, due to which the axes no longer coincide and the final picture deteriorates.
The problem of different eyes

So it has evolved that we have binocular vision. In all primates, the eyes are located on the front of the skull and are oriented parallel to each other. As a rule, binocular vision is a sign of a predator who needs to accurately determine the distance to the prey in order to calculate the jump. In herbivores, eyes are spaced on different sides of the skull to provide maximum visibility and to protect the predator from stalking. In the case of primates, three-dimensional vision, as a rule, serves not to attack the victim, but to accurately determine the distance for jumping from branch to branch. Monkeys that have fallen from a height usually do not reproduce and do not inherit genes.
What does this have to do with today's topic? The most direct. “Gluing” of two slightly different images into one three-dimensional is a function that is sewn into our brain at the level of instinct. However, if the image from different eyes differs more than necessary, then the “program” cannot put everything together. This phenomenon is called amblyopia . The brain, as a rule, “programmatically” discards the defective image from one of the eyes, ignoring it when it perceives the image. As a result, a person receives monocular vision. The causes may vary, but we will consider the option of refractive amblyopia . If a patient has one eye -1.5 D, and the second one is -5.75 D, then the images will be too different to match. Moreover, in such a situation, glasses will not help, as they are located at some distance from the eye and introduce additional distortions.

The standard rule of vision correction is no more than 3 diopters of the difference between lenses for adults and 4 diopters for children. These figures are not absolute dogma and can vary depending on individual tolerance. Contact lenses are almost devoid of this disadvantage, as they are directly adjacent to the cornea and do not have an air gap, and therefore additional distortion. Therefore, with a significant difference in the diopters between the eyes, they are the method of choice from non-operating options.
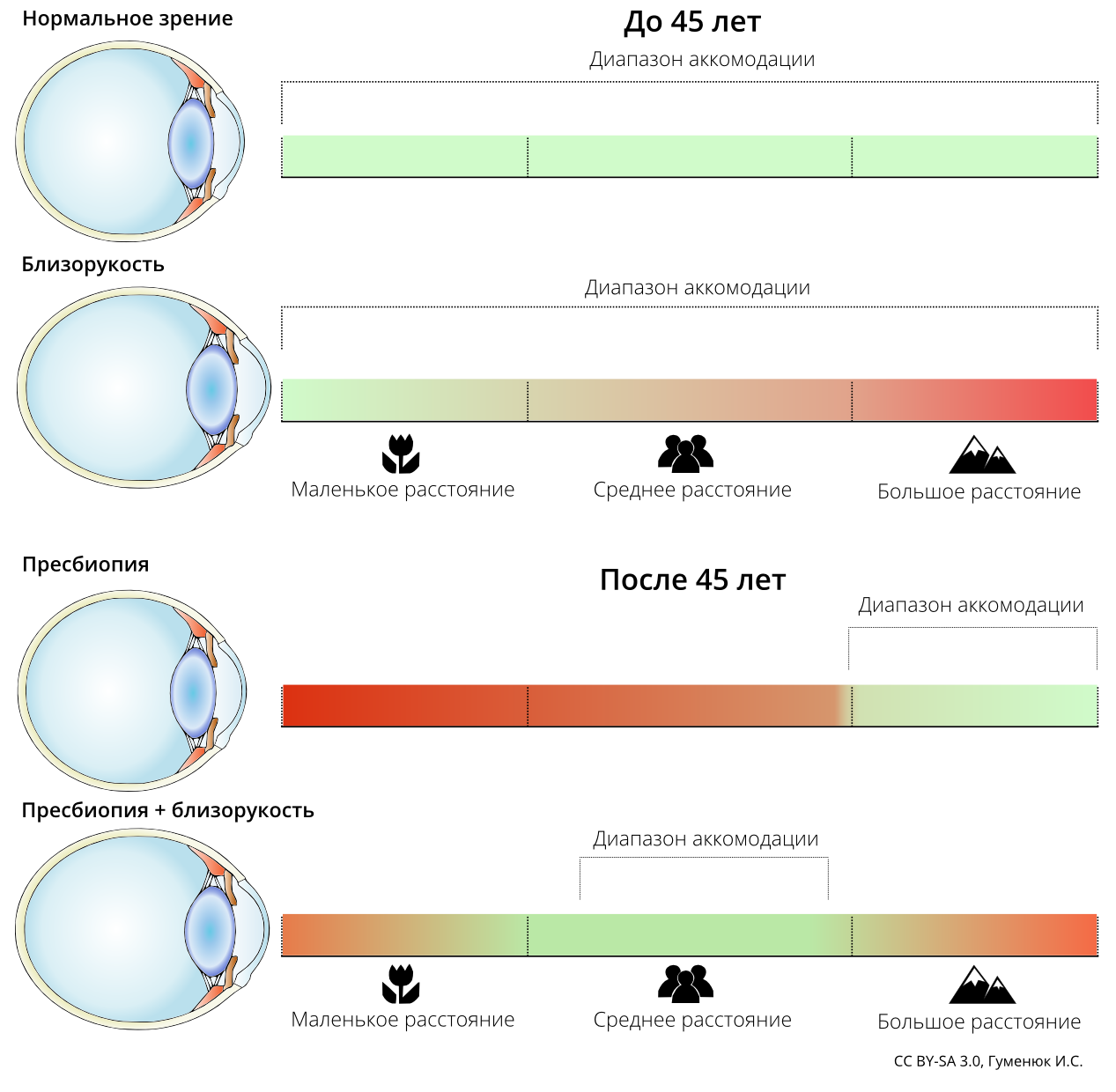
Additional materials: myopia after 45 years
A small digression from the topic. In the previous parts I was asked why people who were short-sighted, after 45 years, see better near. With age, the range of accommodation narrows. However, near-sighted, this range is shifted to the side of close objects. Accommodation, if simplified, is the ability of the lens to change its curvature in order to focus at a different distance.
Vector source for everyone

If you like my illustrations - all source codes are available in vector (Inkscape).
CC BY-SA 3.0 License (CC Attribution - Share Alike)
Sources on Google Drive
To be continued...
UPD
If you have any questions about my publications, do not hesitate. If you are in read-only or you do not have an account on Habré, this is not a problem. In the profile of my contacts in social networks.
Source: https://habr.com/ru/post/218001/
All Articles